AD-Related Dementias Summit 2016: Progress, Aims, Dollars
Quick Links
It may not be obvious from its name, but the National Alzheimer’s Project Act (NAPA) covers related dementias, too—those that go beyond plaques and tangles to involve α-synuclein, TDP-43, and vascular pathologies. The Lewy body, frontotemporal, vascular, and mixed dementias were the focus of the Alzheimer's Disease-Related Dementias (ADRD) 2016 summit held March 29 to 30 at the National Institutes of Health (NIH) in Bethesda, Maryland.
The National Institute on Neurological Disorders and Stroke (NINDS) sponsored this summit, which was coordinated by Roderick Corriveau at NINDS, with David Holtzman of Washington University, St. Louis, overseeing the scientific program. The meeting itself followed six months of preparation, during which about 80 leading scientists, physicians, and administrators were convened around topics and disease areas. Prior to the summit, they updated consensus recommendations from the first ADRD summit in 2013 into a current draft set for 2016.
At the summit, the scientists in these working groups, plus invited experts from several European countries, reported on progress the field had made since 2013. They explained their groups’ new research priorities and solicited public comment. The updated recommendations will guide future federal government spending on research into these types of dementia.
About 400 people—including researchers, representatives of government and nonprofit groups, patients, and caregivers—registered to attend or watch the livecast online. Given the remote option, the auditorium seemed strangely empty at times, yet this physical picture belied a palpable sense of excitement that pervaded the meeting. John Hardy of University College London spoke for many when he told Alzforum, “This is a well-prepared and useful process that helps us determine new research directions and move forward as a field.”
“These summits are not just academic exercises,” added Ronald Petersen, Mayo Clinic, Rochester, Minnesota, who chairs NAPA’s advisory council. “They have a real impact on the process and, at the end of the day, translate into funding opportunities.” Petersen hopes the NIH will issue many more requests for applications (RfAs) a result.
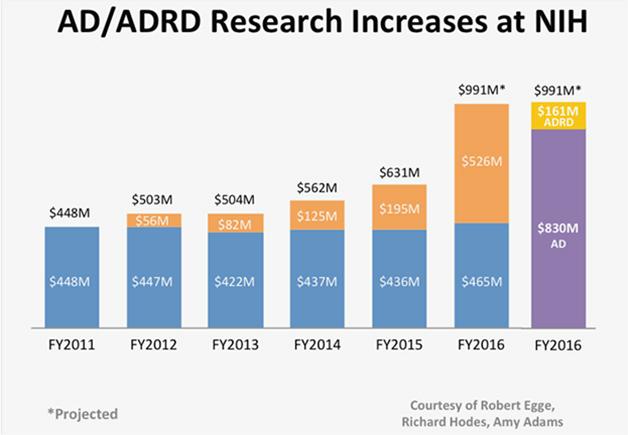
Finally, Funding Rises. Since NAPA was signed into law in 2012, AD-dedicated funds (orange) above the expected (blue) have brought annual federal spending to nearly $1 billion—$830 million for AD and $161 million for ADRD.
It’s a slow process, however. The outcome of this summit will inform the fiscal year 2018 bypass budget for Alzheimer’s research, which will be generated this summer and sent to Congress. The NIH generally issues RfAs once Congressional appropriations come in, hence dollars based directly on this summit appear a long way off. This generated discussion at the summit from researchers who were clamoring for stronger funding sooner. NINDS director Walter Koroshetz encouraged attendees not to wait for future RfAs but to apply now as pay lines at the NINDS and NIA have already begun to rise as a result of NAPA (see NIA Funding Line Policy for FY 2016, FY 2016 NINDS Funding Strategy).
Three years ago, the first 2013 ADRD summit generated 36 recommendations, which factored into a revision of the National Plan to Address Alzheimer’s disease and translated into new RfAs, Petersen said. Government spending got a 60 percent boost in 2016, topping $991 million (see image above; Dec 2015 news story). This money is available now to fund grants, Koroshetz said.
Once finalized, the recommendations from this year’s summit will go to the National Advisory Neurological Disorders and Stroke Council, aka NANDS, and from there to the NAPA council for approval. Together with the recommendations from the 2015 Summit on Alzheimer’s Disease (see Feb 2015 conference series), the ADRD recommendations will become part of the revised National Plan. “Depending on how much actually comes in from Congressional appropriations, we can fund the plan much faster,” Koroshetz told Alzforum. “We always work out the plan for a few years going forward, so that when the money comes in we are ready to fund.”
In its effort to define research priorities, the summit first focused on topics that span individual diseases, such as multiple etiology dementia, health disparities, and the role of non-governmental organizations (NGOs). The program next addressed Lewy body dementias (LBD), frontotemporal lobar degeneration (FTLD), and vascular contributions to cognitive impairment and dementia (VCID, see Part 2 of this series).
Multiple Etiology Dementias
Petersen framed the summit by visually organizing the different molecular etiologies that can underlie clinical impairment. In an old patient, cognitive impairment is likely due to more than one brain pathology, Petersen said, hence the field needs separate biomarkers for each one to define what is driving a given person’s symptoms. Therapy development should proceed on parallel tracks, where some programs target individual component pathologies, such as tau, α-synuclein, or TDP-43, and other programs target common pathways such as axonal degeneration, synaptic dysfunction, proteostasis, or inflammatory mediators, he added. Earlier-onset and genetic dementias are especially valuable for drug development because they tend to be due to a single pathogenic pathway and free of complicating age-related comorbidities, said Holtzman. Multi-etiology dementia will require multiple treatments, many researchers agree.
Diagnosis
Because many dementia patients are unaware of their problem, they often don’t tell their doctors. “Families participate in that, too. It is human nature,” said David Knopman, Mayo Clinic, Rochester, Minnesota. This leads to significant under-diagnosis. “Primary care practices are also problematic: physicians don’t have time for a mental status exam or to talk to families, and they aren’t always familiar with all the various dementing illnesses,” Knopman said.
To help physicians catch cognitive decline early, geriatrician Gwen Windham from the University of Mississippi, Jackson, proposed changes at the primary-care level. She suggested doctors train to recognize these diseases’ red flags and hire social workers who can educate caregivers and connect them with community resources. Windham urged more insurance reimbursement for these services. Video and Internet technology works well to connect rural, underserved communities with expert providers, she said. Technology can also help with cognitive testing, said Sandra Weintraub, Northwestern University, Chicago. Computerized assessments such as Cogstate or the free NIH Toolbox Cognition Battery are suitable to standardize short screenings and automate analysis, Weintraub said. To make this widely used, efforts should be made to beef up tech support, normalize data across diverse populations, and make tests downloadable to avoid security risks of storing personal data on the cloud.
Many physicians remain nihilistic about dementia. But even absent a cure, it is well worth looking for cognitive impairment as part of a wellness exam in older people and making a careful differential diagnosis when something seems amiss, argued Neill Graff-Radford, Mayo Clinic, Jacksonville, Florida. Treatable causes of dementia are quite common, Graff-Radford said: sleep disorders, thiamine, copper, or other nutritional deficiencies, and certain medications, to name a few. The diagnostic criteria for DLB and FTDs work well, and even when the dementia is progressive, symptoms can be controlled early on in some cases. For instance, medications can control sleep disorders, cognitive impairment, and motor problems of DLB, and treating hypertension may slow the progression of vascular dementia.
What’s more, an accurate diagnosis can direct people toward clinical trials and help predict their rate of decline, Graff-Radford said. Physicians should learn and apply the diagnostic criteria for these diseases, and recognize when to refer patients to specialists, he suggested. Consumer health websites could post lists of signs and symptoms that flag treatable causes for dementia.
Ultimately, scientists want to catch and treat ADRD before symptoms arise, said Brad Boeve, Mayo Clinic, Rochester, Minnesota. While biomarkers for preclinical AD are becoming well validated, candidate markers for the early symptomatic stages of DLB and FTD are emerging, as well. In DLB, REM sleep behavior disorder is particularly promising and should be studied for use in screening for this disease. Boeve suggested mining data from the Parkinson’s Progression Markers Initiative and the Parkinson’s Disease Biomarkers Program at NINDS for additional possibilities. In FTD, CSF neurofilament light chain measurement looks promising for symptomatic disease. For presymptomatic FTD, several more years of observational biomarker research with familial cohorts, as underway in GENFI, ARTFL, and LEFFTDS, will yield early biomarkers.
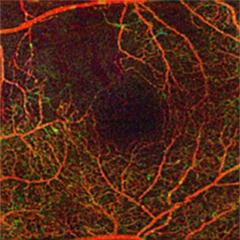
Look Into My Eyes.
Optical coherence tomography-angiography reveals the health of capillaries at higher resolution than MRI. [Courtesy of Amir Kashani, USC Roski Eye Institute.]
For VCID, Helena Chui, University of Southern California, demonstrated the power of imaging techniques to pick up early warning signs. For example, optical coherence tomography-angiopathy can detect capillary weakness that is too subtle for magnetic resonance imaging (see image at right). Dynamic contrast enhancement MRI has been reported to monitor the integrity of the blood-brain barrier (Jan 2015 news).
The Role of NGOs
Because non-AD dementias tend to languish outside the Alzheimer’s spotlight, they can benefit most strongly from the work of dedicated non-governmental organizations, said Susan Dickinson of the Association for Frontotemporal Degeneration (AFTD), Radnor, Pennsylvania. For one thing, these groups draw patients and caregivers into research through education and registries, Dickinson said. “We bring them to the table, get their buy-in on research programs, and get them to inform [study] design,” she told the audience. AFTD is building an FTD Disorders Registry to collect data from patients and caregivers who want to participate in research to accelerate recruitment for clinical trials. AFTD also conducts research. For example, a soon-to-be-published economic burden study estimates the cost FTD imposes on families and society at large. Having these numbers will strengthen researchers’ FTD grant applications, Dickinson said. She particularly emphasized that NGOs should not compete but collaborate in their shared interests, which has not always been the case among dementia philanthropies.
NGOs can also plug gaps in research funding, said Simon Ridley of Alzheimer’s Researcher UK (see image below). Howard Fillit of the Alzheimer’s Drug Discovery Foundation in New York City noted that ADDF supports drug discovery grants that NIH has scored highly but cannot fund. NGO leaders acknowledged that funding young investigators has become a top priority, especially after years of low funding lines have discouraged talented young people to enter the field. “There’s a dearth of researchers and geriatricians from a time when we could not fund Alzheimer’s and related dementias,” said Maria Carrillo, Alzheimer’s Association in Chicago. “We need to support a new generation.”
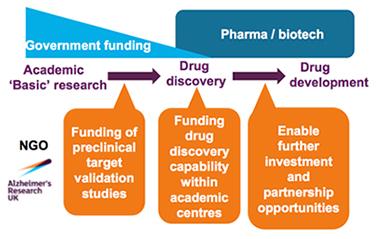
Plugging the Holes.
ARUK supports stages of drug development that tend to be underfunded by government and industry (orange). [Courtesy of Simon Ridley, ARUK.]
The NGO committee recommended regular meetings and better communication between NGOs and the NIH, especially in the years between ADRD summits. “This would enable us to coordinate better, increase the impact of our programs, and develop synergies to make sure the goals are accomplished across the board,” Dickinson said.
ADRDs—A Tower of Babel?
In drawing up their recommendations, scientists and patient advocates agreed that the lack of a unified language to describe different types of dementia is a source of confusion. Even at this meeting, the same diseases are referred to slightly differently, and similar terms describe different disorders, said Angela Taylor of the Lewy Body Dementia Association in Lilburn, Georgia. This is bewildering to patients and their families, said Taylor, who last year was called to serve on the NAPA Advisory Council. Her group called for a task force to develop a lexicon that accommodates the needs of patients, caregivers, healthcare specialists, scientists, and regulators. Such language could improve reporting of symptoms, diagnosis, access to services or therapies, and trial recruitment while increasing public awareness and reducing stigma, Taylor argued. She proposed using a three-tiered system, where a broad umbrella term encompassing cognitive impairment gets broken down by specific syndrome, and is then further divided by disease mechanisms.
Knopman said scientists need to better define the syndromes and etiologies they study and describe them with more precise language. Among Alzheimer’s and Parkinson’s researchers, entrenched debates about terminology have arisen because clinicians classify diseases based on symptoms, whereas pathologists classify them based on molecular pathologies. When clinical diagnoses such as Alzheimer’s disease or mild cognitive impairment are used to enroll treatment trial populations encompassing different underlying etiologies, the trial can be in trouble. Researchers particularly need terms to better define early stages of disease, Knopman said; this will get easier as more biomarkers emerge to subtype causes of dementia. By contrast, patients in an aphasia support group, for example, feel united by their shared symptoms and care less about whether tau or TDP-43 cause them. Hence coming up with a single lexicon that suits disparate groups will be tough, researchers agreed.
Health Disparities in Dementia
Another theme that cut across the summit was health disparities. Non-white, poor, or rural populations tend to be at higher risk for cognitive decline, yet make up only a small percentage of research participants, said Jennifer Manly, Columbia University, New York. Virginia Wadley, University of Alabama at Birmingham, listed some reasons: poor or illiterate people usually lack ties to the research community and some people’s religious beliefs hold them back from research participation. Many clinical trials exclude comorbidities that hit these groups especially hard, and general distrust still lingers from the infamous Tuskegee syphilis study, in which hundreds of African-American men in Alabama were infected with syphilis.
Since the 2013 summit, researchers have made considerable progress in recruiting people from these groups to dementia research, Manly said. Some studies of diverse cohorts have added cognitive and ADRD biomarkers, and the National Institute on Aging will award $12 million in grants for research on heightened dementia risk in disparity populations. However, much work remains, Wadley added. For the 2016 update, her committee called for better tracking of dementia incidence in diverse populations, for development of tools that better assess cognition across cultures and education levels, and for ways to partner with underserved communities. Manly encouraged researchers to dig deeper when they assess population variables. For instance, some studies show that when it comes to education, student-teacher ratios and length of the school year vary widely by region, meaning simply recording years of school may not capture the quality of a person’s education.
How to encourage better participation across race, income level, and geographic regions? Wadley urged scientists to establish relationships with a community before asking members to join a study or donate tissue samples. For instance, they might host health fairs or other events there. They can also offer services that add benefits to research participation, especially for people with limited access to healthcare. They might conduct in-home assessments, provide rides to research centers for brain scans, and return lab reports or a summary of research findings. Including broadly who is affected helps build trust, as well, Wadley said. Several studies have found that these measures go a long way toward improving recruitment (Bress et al., 2016; Barnes et al., 2015).
Lisa Barnes of Rush Medical College in Chicago commented to Alzforum that her center’s outreach to communities of color had yielded more than 300 pledged autopsies from African-American study participants thus far. Sid O’Bryant, University of North Texas, Fort Worth, has also found success with these strategies. “Recruitment of minority or rural populations isn’t that difficult or more expensive,” he said. “It just requires a different effort. You have to become part of the community, hire people from there, and give back.”
See Part 2 of this story for more on the ADRD 2016 summit. Recordings of day 1 and day 2 are available through the NIH Center for Information Technology website.—Gwyneth Dickey Zakaib and Gabrielle Strobel
References
News Citations
- Proposed 2016 Budget Boosts Alzheimer’s Funding By 60 Percent
- At 2016 Summit, Field Tackles AD-Related Dementias One By One
- In Aging Brain, Blood-Brain Barrier Starts Leaking in Hippocampus
Conference Coverage Series Citations
Paper Citations
- Bress AP, Tanner RM, Hess R, Colantonio LD, Shimbo D, Muntner P. Generalizability of SPRINT Results to the U.S. Adult Population. J Am Coll Cardiol. 2016 Feb 9;67(5):463-72. Epub 2015 Nov 9 PubMed.
- Barnes LL, Leurgans S, Aggarwal NT, Shah RC, Arvanitakis Z, James BD, Buchman AS, Bennett DA, Schneider JA. Mixed pathology is more likely in black than white decedents with Alzheimer dementia. Neurology. 2015 Aug 11;85(6):528-34. Epub 2015 Jul 15 PubMed.
External Citations
Further Reading
Papers
- Kashani AH, Lee SY, Moshfeghi A, Durbin MK, Puliafito CA. OPTICAL COHERENCE TOMOGRAPHY ANGIOGRAPHY OF RETINAL VENOUS OCCLUSION. Retina. 2015 Nov;35(11):2323-31. PubMed.
Annotate
To make an annotation you must Login or Register.
Comments
No Available Comments
Make a Comment
To make a comment you must login or register.