In Amyloid Cascade, Do Reactive Astrocytes Bridge Plaques and Tangles?
Quick Links
Why do some people with amyloid plaques decline, while others do not? In the May 29 Nature Medicine, researchers led by Tharick Pascoal at the University of Pittsburgh laid some of the blame on reactive astrocytes. Among cognitively healthy people with amyloid plaques, only those whose astrocytes were activated, as judged by plasma GFAP, accumulated tau pathology. The relationship held in three separate cohorts, and when using different ways to measure amyloid and tau. The findings hint that astrocytes drive tangle formation, the authors said. “GFAP positivity could help us identify people with brain amyloid who are fated to develop tau pathology,” Pascoal told Alzforum.
- In preclinical AD, tau phosphorylation only occurs when plasma GFAP rises.
- This marker of reactive astrocytes predicted tangle spread over time.
- Can this fairly broad astrocyte marker help predict clinical progression?
Commenters deemed the evidence convincing for a link between GFAP and p-tau181. “While correlation does not mean causation, the finding … suggests that reactive astrocytes play a central role at the earliest stages of the AD pathophysiological process,” Alberto Serrano-Pozo at Massachusetts General Hospital, Charlestown, wrote to Alzforum. Nonetheless, they said questions remain, such as the direction of that association, the effect of co-morbidities, and the specificity of the marker itself. “More research into this important area is warranted,” said Jeffrey Dage at Indiana University, Indianapolis (comments below).
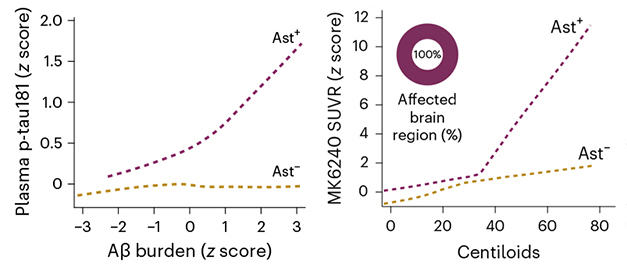
Astrocyte as Enabler. In cognitively healthy people, plasma p-tau181 (left), and tau PET in Braak 1 regions (right), rise along with plaque burden only in people whose astrocytes are in a reactive state (Ast+). [Courtesy of Bellaver et al., Nature Medicine.]
Scientists have long known that reactive astrocytes appear around amyloid plaques early in AD (Pike et al., 1995; Kumar et al., 2021). More recently, studies have correlated high plasma GFAP with plaques in the brain (Mar 2021 conference news; Chatterjee et al., 2021; Pereira et al., 2021). Curiously, one study reported that GFAP in plasma predicts the presence of brain amyloid more accurately than does GFAP in cerebrospinal fluid (Benedet et al., 2021).
To find out how GFAP relates to other AD biomarkers, first author Bruna Bellaver compared cognitively healthy people in three observational cohorts: the TRIAD study at McGill University, a research cohort at Pittsburgh, and the population-based MYHAT cohort in Pittsburgh. Together, the sample comprised 1,016 people, average of 70 years old. Bellaver and colleagues classified each participant as positive (Ast+) or negative (Ast-) for reactive astrocytes, setting the cutoff for plasma GFAP at two standard deviations above the average in amyloid-negative participants. Among the 294 amyloid-positive participants, 108 were Ast+ by this measure, 186 were Ast-.
In the former, plasma p-tau181 was high, while in the latter, levels were as low as in amyloid-negative controls. Importantly, only in Ast+ people did plaque burden correlate with p-tau181 (see graph above). The effect size was large, with a Cohen’s d of 0.80. Likewise, in a subgroup of 147 participants who had a tau PET scan with the MK6240 tracer, tangle load in the earliest Braak regions correlated with amyloid load only in the Ast+ group, again suggesting that astrocytes mediate this association.
In the Ast+ group, the association between plaque and p-tau181 was stronger in men than women. Previous studies have reported higher overall tangle burden in women than men (Aug 2018 conference news; Feb 2019 news; Nov 2019 news). The new data suggest that reactive astrocytes may play a bigger role in men, while other mechanisms are at work in women, Pascoal noted.
How might astrocytes influence tangle formation? Previous cell culture and animal studies have found that activated astrocytes release factors, such as cytokines and adenosine triphosphatase, that trigger tau phosphorylation in neurons (Garwood et al., 2011; Litvinchuk et al., 2018; Mann et al., 2022). Pascoal plans to probe mechanisms in the human brain by analyzing single-cell RNA-Seq in postmortem tissue to identify genes highly expressed in reactive astrocytes.
Serrano-Pozo noted that in the AD brain, reactive astrocytes wrap their processes around plaques, tangles, and dystrophic neurites containing phosphorylated tau. “Reactive astrocytes are uniquely positioned to link Aβ and p-tau pathologies,” he said. Others noted caveats. Rik Ossenkoppele and Emma Coomans at Amsterdam University Medical Center pointed out that plasma markers often track up or down in concert within individuals, and that more work will be needed to show a causal effect (comment below).

Tangle Driver? In people positive for reactive astrocytes (bottom), tangles increased (red) each year, while those negative for reactive astrocytes (top) had little change. [Courtesy of Bellaver et al., Nature Medicine.]
What happens over time? The study had longitudinal data on 71 participants. In them, baseline plaque burden predicted tangle spread over two years only in those who were Ast+ (image at right). This implies that screening for plasma GFAP could enrich clinical trials for people whose disease is most likely to progress, Pascoal suggested. If the findings hold up, he believes reactive astrocytes could eventually be incorporated into the definition of preclinical AD.
Beau Ances at Washington University in St. Louis agreed, noting that the ATN staging scheme could be updated to include an inflammatory marker. On the other hand, Oskar Hansson and Gemma Salvadó at Lund University, Sweden, said that in their hands, plasma GFAP does not improve upon high-performing plasma p-tau assays that detect plaques and tangles. “That said, we think plasma GFAP is a very interesting outcome marker in interventional studies evaluating the effects of new disease-modifying or lifestyle interventions,” they wrote. Others cautioned that GFAP lacks specificity. “This is why it is important that we shift toward the use of bona fide reactive astrocyte markers that are never expressed by astrocytes in a physiological setting, such as Lcn2, Serpina3n, and many others identified by recent sequencing efforts,” wrote Shane Liddelow, New York University (comments below).
Pascoal and colleagues are now broadening their study by including racially diverse cohorts with co-morbidities such as cardiovascular disease. They will also examine later stages of disease to determine how long into the disease this early stage relationship between plaques, tangles, and reactive astrocytes occurs.—Madolyn Bowman Rogers
References
News Citations
- Astroglial Markers Poised for Stardom?
- Do Brain Changes at Menopause Make Women More Prone to Alzheimer’s?
- Is a Woman’s Brain More Susceptible to Tau Pathology?
- ApoE4 and Tau in Alzheimer’s: Worse Than We Thought? Especially in Women
Paper Citations
- Pike CJ, Cummings BJ, Cotman CW. Early association of reactive astrocytes with senile plaques in Alzheimer's disease. Exp Neurol. 1995 Apr;132(2):172-9. PubMed.
- Kumar A, Fontana IC, Nordberg A. Reactive astrogliosis: A friend or foe in the pathogenesis of Alzheimer's disease. J Neurochem. 2021 Dec 20; PubMed.
- Chatterjee P, Pedrini S, Stoops E, Goozee K, Villemagne VL, Asih PR, Verberk IM, Dave P, Taddei K, Sohrabi HR, Zetterberg H, Blennow K, Teunissen CE, Vanderstichele HM, Martins RN. Plasma glial fibrillary acidic protein is elevated in cognitively normal older adults at risk of Alzheimer's disease. Transl Psychiatry. 2021 Jan 11;11(1):27. PubMed.
- Pereira JB, Janelidze S, Smith R, Mattsson-Carlgren N, Palmqvist S, Teunissen CE, Zetterberg H, Stomrud E, Ashton NJ, Blennow K, Hansson O. Plasma GFAP is an early marker of amyloid-β but not tau pathology in Alzheimer's disease. Brain. 2021 Dec 16;144(11):3505-3516. PubMed.
- Benedet AL, Milà-Alomà M, Vrillon A, Ashton NJ, Pascoal TA, Lussier F, Karikari TK, Hourregue C, Cognat E, Dumurgier J, Stevenson J, Rahmouni N, Pallen V, Poltronetti NM, Salvadó G, Shekari M, Operto G, Gispert JD, Minguillon C, Fauria K, Kollmorgen G, Suridjan I, Zimmer ER, Zetterberg H, Molinuevo JL, Paquet C, Rosa-Neto P, Blennow K, Suárez-Calvet M, Translational Biomarkers in Aging and Dementia (TRIAD) study, Alzheimer’s and Families (ALFA) study, and BioCogBank Paris Lariboisière cohort. Differences Between Plasma and Cerebrospinal Fluid Glial Fibrillary Acidic Protein Levels Across the Alzheimer Disease Continuum. JAMA Neurol. 2021 Dec 1;78(12):1471-1483. PubMed.
- Garwood CJ, Pooler AM, Atherton J, Hanger DP, Noble W. Astrocytes are important mediators of Aβ-induced neurotoxicity and tau phosphorylation in primary culture. Cell Death Dis. 2011;2:e167. PubMed.
- Litvinchuk A, Wan YW, Swartzlander DB, Chen F, Cole A, Propson NE, Wang Q, Zhang B, Liu Z, Zheng H. Complement C3aR Inactivation Attenuates Tau Pathology and Reverses an Immune Network Deregulated in Tauopathy Models and Alzheimer's Disease. Neuron. 2018 Dec 19;100(6):1337-1353.e5. Epub 2018 Nov 8 PubMed.
- Mann CN, Devi SS, Kersting CT, Bleem AV, Karch CM, Holtzman DM, Gallardo G. Astrocytic α2-Na+/K+ ATPase inhibition suppresses astrocyte reactivity and reduces neurodegeneration in a tauopathy mouse model. Sci Transl Med. 2022 Feb 16;14(632):eabm4107. PubMed.
Further Reading
News
- A Putrid Problem: Astrocytic Urea Cycle in Alzheimer’s?
- Astrocyte Reactivity: Opposing States Emerge
- Hyperconnectivity in Cingulate Precedes Amyloid. Astrocytes to Blame?
- Aβ Clearance—The Untapped Potential of Astrocytes?
- ELOVL Hurts—Enzyme Makes Lipids That Turn Astrocytes Toxic
- Reactive Astrocytes Boot Basic, Dysfunctional Lysosomes
- Squelching ApoE in Astrocytes of Tau-Ravaged Mice Dampens Degeneration
- Does Astrocyte Tau Cause Dementia?
Primary Papers
- Bellaver B, Povala G, Ferreira PC, Ferrari-Souza JP, Leffa DT, Lussier FZ, Benedet AL, Ashton NJ, Triana-Baltzer G, Kolb HC, Tissot C, Therriault J, Servaes S, Stevenson J, Rahmouni N, Lopez OL, Tudorascu DL, Villemagne VL, Ikonomovic MD, Gauthier S, Zimmer ER, Zetterberg H, Blennow K, Aizenstein HJ, Klunk WE, Snitz BE, Maki P, Thurston RC, Cohen AD, Ganguli M, Karikari TK, Rosa-Neto P, Pascoal TA. Astrocyte reactivity influences amyloid-β effects on tau pathology in preclinical Alzheimer's disease. Nat Med. 2023 Jul;29(7):1775-1781. Epub 2023 May 29 PubMed.
Annotate
To make an annotation you must Login or Register.
Comments
Massachusetts General Hospital / Harvard Medical School
Bruna Bellaver and colleagues have authored a tour de force, multicenter, AD biomarker study with 1,000+ participants from three clinical sites that expands our understanding of plasma GFAP as a biomarker of reactive astrogliosis in early stage AD. While correlation does not mean causation, the finding of a stronger association between Aβ and p-tau levels in cognitively unimpaired individuals with high GFAP plasma levels (i.e., Ast+) relative to those with low GFAP plasma levels (or Ast-) suggests that reactive astrocytes play a central role at the earliest stages of the AD pathophysiological process.
In postmortem brain specimens, reactive GFAP+ astrocytes can be found not only wrapping fibrillar Aβ plaques—many of them containing p-tau+ dystrophic neurites—but also in the vicinity of neurofibrillary tangles (Serrano-Pozo et al., 2011). Moreover, astrocytes structurally contribute with their fine processes to the tripartite excitatory synapses. Thus, reactive astrocytes are uniquely positioned to link Aβ and p-tau pathologies and to facilitate the transsynaptic spreading of p-tau (Montal et al., 2022; Serrano-Pozo et al., 2022).
Undoubtedly, it is a very exciting time in the AD biomarker field. Plasma GFAP level is a proxy for reactive astrogliosis, thought to reflect the intermediate filament cytoskeleton hypertrophy of reactive astrocytes in the brain. While a binary classification of individuals as Ast+ or Ast- based on a plasma GFAP level cutoff may become clinically useful, we think of reactive astrogliosis as a continuous phenotypic change, from homeostatic to reactive states through intermediate transitional states (Serrano-Pozo et al., 2022; Serrano-Pozo et al., 2013; Muñoz-Castro, 2022), and, as a complex phenomenon with multiple functional gains and losses beyond GFAP upregulation (Serrano-Pozo et al., 2022; Viejo et al., 2022; Escartin et al., 2021).
Thus, the quest for fluid biomarkers of reactive astrogliosis should not stop with GFAP and CHI3L1/YKL-40 (Bellaver et al., 2021), rather, it should go on to provide us with a fuller picture of this complexity. In addition, PET imaging biomarkers of reactive astrogliosis are much needed to better understand the spatiotemporal relationship between reactive astrocytes and Aβ plaques and neurofibrillary tangles along the normal aging-AD continuum (Villemagne et al., 2022; Chatterjee et al., 2023). Lastly, more experimental studies in AD mouse models are needed to elucidate the likely bidirectional effects between reactive astrocytes and both pathologies.
References:
Serrano-Pozo A, Mielke ML, Gómez-Isla T, Betensky RA, Growdon JH, Frosch MP, Hyman BT. Reactive glia not only associates with plaques but also parallels tangles in Alzheimer's disease. Am J Pathol. 2011 Sep;179(3):1373-84. PubMed.
Montal V, Diez I, Kim CM, Orwig W, Bueichekú E, Gutiérrez-Zúñiga R, Bejanin A, Pegueroles J, Dols-Icardo O, Vannini P, El-Fakhri G, Johnson KA, Sperling RA, Fortea J, Sepulcre J. Network Tau spreading is vulnerable to the expression gradients of APOE and glutamatergic-related genes. Sci Transl Med. 2022 Jul 27;14(655):eabn7273. PubMed.
Serrano-Pozo A, Li Z, Woodbury ME, Munoz-Castro C, Wachter A, Jayakumar R, Bryant AG, Noori A, Welikovitch LA, Hu M, Liao F, Lin G, Pastika T, Tamm J, Abdourahman A, Kwon T, Bennett RE, Talanian RV, Biber K, Karran EH, Hyman BT, Das S. Astrocyte transcriptomic changes along the spatiotemporal progression of Alzheimer's disease. 2022 Dec 07 10.1101/2022.12.03.518999 (version 1) bioRxiv.
Serrano-Pozo A, Gómez-Isla T, Growdon JH, Frosch MP, Hyman BT. A phenotypic change but not proliferation underlies glial responses in Alzheimer disease. Am J Pathol. 2013 Jun;182(6):2332-44. PubMed.
Muñoz-Castro C, Noori A, Magdamo CG, Li Z, Marks JD, Frosch MP, Das S, Hyman BT, Serrano-Pozo A. Cyclic multiplex fluorescent immunohistochemistry and machine learning reveal distinct states of astrocytes and microglia in normal aging and Alzheimer's disease. J Neuroinflammation. 2022 Feb 2;19(1):30. PubMed.
Viejo L, Noori A, Merrill E, Das S, Hyman BT, Serrano-Pozo A. Systematic review of human post-mortem immunohistochemical studies and bioinformatics analyses unveil the complexity of astrocyte reaction in Alzheimer's disease. Neuropathol Appl Neurobiol. 2022 Feb;48(1):e12753. Epub 2021 Aug 17 PubMed.
Escartin C, Galea E, Lakatos A, O'Callaghan JP, Petzold GC, Serrano-Pozo A, Steinhäuser C, Volterra A, Carmignoto G, Agarwal A, Allen NJ, Araque A, Barbeito L, Barzilai A, Bergles DE, Bonvento G, Butt AM, Chen WT, Cohen-Salmon M, Cunningham C, Deneen B, De Strooper B, Díaz-Castro B, Farina C, Freeman M, Gallo V, Goldman JE, Goldman SA, Götz M, Gutiérrez A, Haydon PG, Heiland DH, Hol EM, Holt MG, Iino M, Kastanenka KV, Kettenmann H, Khakh BS, Koizumi S, Lee CJ, Liddelow SA, MacVicar BA, Magistretti P, Messing A, Mishra A, Molofsky AV, Murai KK, Norris CM, Okada S, Oliet SH, Oliveira JF, Panatier A, Parpura V, Pekna M, Pekny M, Pellerin L, Perea G, Pérez-Nievas BG, Pfrieger FW, Poskanzer KE, Quintana FJ, Ransohoff RM, Riquelme-Perez M, Robel S, Rose CR, Rothstein JD, Rouach N, Rowitch DH, Semyanov A, Sirko S, Sontheimer H, Swanson RA, Vitorica J, Wanner IB, Wood LB, Wu J, Zheng B, Zimmer ER, Zorec R, Sofroniew MV, Verkhratsky A. Reactive astrocyte nomenclature, definitions, and future directions. Nat Neurosci. 2021 Mar;24(3):312-325. Epub 2021 Feb 15 PubMed.
Bellaver B, Ferrari-Souza JP, Uglione da Ros L, Carter SF, Rodriguez-Vieitez E, Nordberg A, Pellerin L, Rosa-Neto P, Leffa DT, Zimmer ER. Astrocyte Biomarkers in Alzheimer Disease: A Systematic Review and Meta-analysis. Neurology. 2021 May 5; PubMed.
Villemagne VL, Harada R, Dore V, Furumoto S, Mulligan R, Kudo Y, Burnham S, Krishnadas N, Bourgeat P, Xia Y, Laws S, Bozinovski S, Huang K, Ikonomovic MD, Fripp J, Yanai K, Okamura N, Rowe CC. Assessing reactive astrogliosis with 18F-SMBT-1 across the Alzheimer's disease spectrum. J Nucl Med. 2022 Jan 27; PubMed.
Chatterjee P, Doré V, Pedrini S, Krishnadas N, Thota R, Bourgeat P, Ikonomovic MD, Rainey-Smith SR, Burnham SC, Fowler C, Taddei K, Mulligan R, Ames D, Masters CL, Fripp J, Rowe CC, Martins RN, Villemagne VL, and for the AIBL Research Group. Plasma Glial Fibrillary Acidic Protein Is Associated with 18F-SMBT-1 PET: Two Putative Astrocyte Reactivity Biomarkers for Alzheimer's Disease. J Alzheimers Dis. 2023;92(2):615-628. PubMed.
Indiana University School Of Medicine
Glial cell involvement in AD was noted in the earliest observations of Dr. Alzheimer. It is not surprising that a marker of astrocyte activation, GFAP, is elevated in the plasma from patients with evidence of amyloid pathology. The challenge is trying to work out what it means given the complicated and multifunctional role of astrocytes in the brain. Bellaver et al. set out to determine if elevated GFAP, and its interaction with amyloid pathology, are associated with levels of phosphorylated tau (p-tau181) in preclinical AD. They demonstrated convincing evidence for this association.
The authors suggest that adding astrocyte activation (Ast) to the ATN biomarker scheme could provide a more granular classification in preclinical stages. However, a more granular classification will dilute effects across a larger number of groups, requiring much larger sample sizes. This is an important area for research, but one in which sample size will need to be carefully considered.
It is also important to consider the role of the blood-brain barrier (BBB) when interpreting plasma GFAP levels and their relationship with other blood biomarkers. One alternate hypothesis is that activated astrocytes associated with plaque and having elevated GFAP are also associated with BBB dysfunction. This could be through similar signaling, or more directly influenced by the presence of cerebral amyloid angiopathy. This BBB dysfunction could result in “leaking” of many proteins from the brain into the vasculature, including GFAP and p-tau, which would appear to be associated due to the common path.
This is just an alternate hypothesis, indicating more work needs to be done to understand the associations and interactions between pathologies and the biomarkers that we can measure. It would be good to develop a marker that could reliably inform on the status of the BBB.
Along those BBB lines, vascular disease is higher in men and might account for the observed sex differences. It would be good to know if the cardiovascular disease cohorts that were used also showed a gender effect in CVD risk factors. Certainly, more research into this important area is warranted and Bellaver et al. have successfully demonstrated how these important studies can be accomplished.
VU University Medical Center
Amsterdam UMC, VUMC
This interesting study addresses the important question of why some individuals with Aβ pathology do not exhibit detectable tau pathology in their brains. In this large, multicohort study, including 1,016 cognitively unimpaired individuals, the authors observed that—as expected—plasma p-tau181 increased as a function of Aβ burden (measured using either plasma Aβ42/40 or Aβ-PET). However, this was only the case in individuals with a positive plasma GFAP measure, which may reflect increased astrocyte reactivity. The authors provided several additional analyses to investigate the robustness of this effect, including cohort-stratified analyses, assessment of different plasma GFAP thresholds, assessment of other plasma p-tau isoforms, and (in a small subset) assessment of tau-PET, which all showed largely similar results.
The research question addressed is highly relevant for the field, because it could provide novel insights into disease mechanisms and help identify individuals at risk for developing tau tangles in the brain. This is important because tau-PET positivity in preclinical AD populations is associated with rapid future clinical progression (Ossenkoppele et al., 2022; Strikwerda-Brown et al., 2022).
However, some caution about the interpretation of the results is warranted. First, it is unclear whether, and to what degree, GFAP concentrations in plasma truly resemble astrocyte reactivity in the brain. To the best of our knowledge, there is currently no conclusive antemortem versus postmortem evidence regarding the measurement properties of plasma GFAP.
Second, different plasma markers (even those from distinct molecular classes) tend to co-vary within individuals. This raises the question of whether the observed moderating effect is unique to plasma GFAP/reactive astrocytes, constitutes a combination of processes (e.g., microglia activation, synaptic alterations, vascular changes etc.), or could even represent a generic signal of disrupted brain homeostasis?
Third, the primary tau-biomarker used in this study (plasma p-tau181) has been shown to reflect a mix of Aβ and tau pathological changes in the brain (Salvadó et al., 2023), and is therefore not a “pure” marker of tau tangle load in the brain. It will be interesting to examine these associations in larger tau-PET cohorts, which measure more mature insoluble tau aggregates. Our interpretation of the initial tau-PET data presented in the paper is that the moderating effect of plasma GFAP on the relationship between Aβ burden and the tau biomarker seems more pronounced for plasma p-tau than for tau-PET. Fourth, the directionality of the observed associations is still open, as alternative pathways—for example, changes in plasma GFAP occurring downstream of [Aβ-related] changes in [soluble] tau pathology—cannot be disregarded.
All told, this paper describes a highly interesting and well-described study. It highlights plasma GFAP as an interesting marker of disease progression, however, the moderating effect of astrocyte reactivity on the association between Aβ and tau remains to be better understood. We look forward to future work including other biomarkers of astrocyte reactivity (e.g., PET markers), which may provide further insights on the complex links between Aβ and tau.
References:
Ossenkoppele R, Pichet Binette A, Groot C, Smith R, Strandberg O, Palmqvist S, Stomrud E, Tideman P, Ohlsson T, Jögi J, Johnson K, Sperling R, Dore V, Masters CL, Rowe C, Visser D, van Berckel BN, van der Flier WM, Baker S, Jagust WJ, Wiste HJ, Petersen RC, Jack CR Jr, Hansson O. Amyloid and tau PET-positive cognitively unimpaired individuals are at high risk for future cognitive decline. Nat Med. 2022 Nov;28(11):2381-2387. Epub 2022 Nov 10 PubMed.
Salvadó G, Ossenkoppele R, Ashton NJ, Beach TG, Serrano GE, Reiman EM, Zetterberg H, Mattsson-Carlgren N, Janelidze S, Blennow K, Hansson O. Specific associations between plasma biomarkers and postmortem amyloid plaque and tau tangle loads. EMBO Mol Med. 2023 May 8;15(5):e17123. Epub 2023 Mar 13 PubMed.
Strikwerda-Brown C, Hobbs DA, Gonneaud J, St-Onge F, Binette AP, Ozlen H, Provost K, Soucy JP, Buckley RF, Benzinger TL, Morris JC, Villemagne VL, Doré V, Sperling RA, Johnson KA, Rowe CC, Gordon BA, Poirier J, Breitner JC, Villeneuve S, PREVENT-AD, HABS, and AIBL Research Groups. Association of Elevated Amyloid and Tau Positron Emission Tomography Signal With Near-Term Development of Alzheimer Disease Symptoms in Older Adults Without Cognitive Impairment. JAMA Neurol. 2022 Oct 1;79(10):975-985. PubMed.
Lund University
Lund University
Studies on modulators of amyloid-associated accumulation of tau are most warranted, and this study is a truly great example, showing that there might be a relationship between active astrocytes and a buildup of tau tangle pathology. Among the strong points of the study are the big sample size and the inclusion of three different cohorts, which support the generalizability of the results. However, the study is, of course, observational in nature and therefore we should be very careful not to make strong conclusions regarding causality, i.e., we cannot say that the study provides solid evidence that Aβ pathology results in reactive astrocytes, which in turn worsen tau pathology.
Alternatively, activated astrocytes could simply be a reaction to neuronal degeneration associated with Aβ and/or tangle pathology. A recent neuropathology-based study found that plasma GFAP levels are more associated with the density of tau tangle pathology than amyloid plaque load (Salvadó et al., 2023). That said, this current study is a great argument to perform further mechanistic studies using cell and animal models in this area of research.
Another question is, what does increased plasma GFAP mean physiologically? Although GFAP is mainly released by activated astrocytes in the brain, it is still somewhat controversial whether its concentrations in the blood are strictly related to only astrocytic reactivity. Previous studies have already suggested important differences between GFAP when measured in CSF and in plasma (Benedet al., 2021). Although differences in pre-analytical factors between the two measures could explain some of the differences (Simrén et al., 2022), more detailed analyses are needed to fully understand this biomarker.
Importantly, plasma GFAP could be considered for use in clinical practice and in trials. However, we have not yet found that plasma GFAP provides any independent information beyond high-performing plasma p-tau assays when detecting amyloid or tau pathology in cross-sectional settings. Similarly, we have not seen that plasma GFAP contributes to plasma p-tau217 when predicting future accumulation of tau aggregates or when predicting subsequent cognitive decline in either preclinical AD (Mattsson-Carlgren et al., 2023) or in cognitively impaired people (Smith et al., 2023).
These results might question the role of plasma GFAP as an important marker in the diagnostic or prognostic workup of Alzheimer’s disease in clinical practice. That said, we think plasma GFAP is a very interesting outcome marker in interventional studies that evaluate the effects of new disease-modifying interventions or lifestyle interventions.
References:
Salvadó G, Ossenkoppele R, Ashton NJ, Beach TG, Serrano GE, Reiman EM, Zetterberg H, Mattsson-Carlgren N, Janelidze S, Blennow K, Hansson O. Specific associations between plasma biomarkers and postmortem amyloid plaque and tau tangle loads. EMBO Mol Med. 2023 May 8;15(5):e17123. Epub 2023 Mar 13 PubMed.
Benedet AL, Milà-Alomà M, Vrillon A, Ashton NJ, Pascoal TA, Lussier F, Karikari TK, Hourregue C, Cognat E, Dumurgier J, Stevenson J, Rahmouni N, Pallen V, Poltronetti NM, Salvadó G, Shekari M, Operto G, Gispert JD, Minguillon C, Fauria K, Kollmorgen G, Suridjan I, Zimmer ER, Zetterberg H, Molinuevo JL, Paquet C, Rosa-Neto P, Blennow K, Suárez-Calvet M, Translational Biomarkers in Aging and Dementia (TRIAD) study, Alzheimer’s and Families (ALFA) study, and BioCogBank Paris Lariboisière cohort. Differences Between Plasma and Cerebrospinal Fluid Glial Fibrillary Acidic Protein Levels Across the Alzheimer Disease Continuum. JAMA Neurol. 2021 Dec 1;78(12):1471-1483. PubMed.
Simrén J, Weninger H, Brum WS, Khalil S, Benedet AL, Blennow K, Zetterberg H, Ashton NJ. Differences between blood and cerebrospinal fluid glial fibrillary Acidic protein levels: The effect of sample stability. Alzheimers Dement. 2022 Oct;18(10):1988-1992. Epub 2022 Sep 14 PubMed.
Simrén J, Weninger H, Brum WS, Khalil S, Benedet AL, Blennow K, Zetterberg H, Ashton NJ. Differences between blood and cerebrospinal fluid glial fibrillary Acidic protein levels: The effect of sample stability. Alzheimers Dement. 2022 Oct;18(10):1988-1992. Epub 2022 Sep 14 PubMed.
Mattsson-Carlgren N, Salvadó G, Ashton NJ, Tideman P, Stomrud E, Zetterberg H, Ossenkoppele R, Betthauser TJ, Cody KA, Jonaitis EM, Langhough R, Palmqvist S, Blennow K, Janelidze S, Johnson SC, Hansson O. Prediction of Longitudinal Cognitive Decline in Preclinical Alzheimer Disease Using Plasma Biomarkers. JAMA Neurol. 2023 Apr 1;80(4):360-369. PubMed.
Smith R, Cullen NC, Pichet Binette A, Leuzy A, Blennow K, Zetterberg H, Klein G, Borroni E, Ossenkoppele R, Janelidze S, Palmqvist S, Mattsson-Carlgren N, Stomrud E, Hansson O, Alzheimer's Disease Neuroimaging Initiative. Tau-PET is superior to phospho-tau when predicting cognitive decline in symptomatic AD patients. Alzheimers Dement. 2023 Jun;19(6):2497-2507. Epub 2022 Dec 14 PubMed.
NYU Langone
With 1,000 patients included, this is a well-powered study. Do the profound changes in GFAP levels in the serum mean something about AD pathology/progression? One hundred percent. Do they definitively mean astrocyte reactivity states are involved? I'm not 100 percent sure, yet. While it is true that GFAP levels can increase when astrocytes enter a reactive state, the heterogeneity of GFAP levels throughout the CNS remains a complicating factor in interpreting these data. This is why it is important that we shift toward the use of bona fide reactive astrocyte markers that are never expressed by astrocytes in a physiological setting, such as Lcn2, Serpina3n, and many others identified by recent sequencing efforts.
An additional complication is the lack of fidelity for GFAP as a pure astrocyte marker. Several CNS cell types express Gfap, e.g. astrocytes, Mueller glia, and radial glia, making the protein's use as a single marker difficult. In the periphery, many tissue-specific glial cells express Gfap or stain for GFAP, e.g., enteric glia, non-myelinating Schwann cells, etc. This makes it difficult to be sure that plasma GFAP is solely from astrocytes and not from other CNS or non-CNS glia.
In any case, this study nicely highlights how a focus on pure pathology/pathogenic proteins, or neuron health/numbers is only giving us a small part of the AD story. Importantly, the GFAP plasma level (high versus low) provides an intriguing way to isolate subpopulations of patients who have otherwise been aggregated together. These discoveries are likely to uncover additional novel components of the AD puzzle moving forward.
To my mind, the most important piece here is that, as a field, we need to focus more on the early non-neuronal markers of disease. That there is such a profound and early change in plasma GFAP levels highlights, once again, that non-neuronal cells, wherever they are in the body, are likely not simply responding to late-stage pathology, but that they are integral components of the early pathogenesis of the disease.
VU University Medical Center
GFAP is gaining more and more interest as a biomarker for Alzheimer’s disease and other dementias. While previous studies already indicated the prognostic value of GFAP, e.g., in cognitively unimpaired individuals in memory clinics (Verberk et al., 2021; Chatterjee et al., 2021), or a twin cohort (Den Braber, Brain Comm in press) for cognitive decline and dementia, a specific interaction with amyloid positivity was suggested by recent data in the DIAN cohort, showing prognostic value for clinical decline and atrophy especially in amyloid-positive individuals (Chatterjee et al., 2022).
Pascaol and collaborators took a different approach, studying whether GFAP positivity influenced the correlation between amyloid and tau. Their work is convincing, by showing a correlation between amyloid and tau pathology in GFAP-positive individuals consistently across data from three independent cohorts and several measures of amyloid and tau pathology (e.g., PET imaging, fluid biomarkers, different p-tau isoforms).
What questions remain? Comparison with astrocyte imaging results would be desirable. Next, GFAP is currently the only available plasma marker for astrocyte reactivity. It would be great to increase the understanding of astrocyte reactivity via other functional biomarkers. Microglia activation is another relevant glial cell that can mediate the interaction between amyloid and tau pathology. The authors measured one biomarker, sTREM2, which showed no such effect. This could be due to several factors, including fold change within the AD population, or the U-shape of this marker along the AD continuum, and thus the role of microglia cannot be excluded based on this marker alone.
All in all, this study forms a good basis for addressing the question of whether there is an exclusive need of GFAP as mediator between amyloid aggregation and tau pathology, which should ideally be proven by expansion of direct experimental cellular models.
References:
Verberk IM, Laarhuis MB, van den Bosch KA, Ebenau JL, van Leeuwenstijn M, Prins ND, Scheltens P, Teunissen CE, van der Flier WM. Serum markers glial fibrillary acidic protein and neurofilament light for prognosis and monitoring in cognitively normal older people: a prospective memory clinic-based cohort study. Lancet Healthy Longev. 2021 Feb;2(2):e87-e95. Epub 2021 Jan 19 PubMed.
Chatterjee P, Pedrini S, Stoops E, Goozee K, Villemagne VL, Asih PR, Verberk IM, Dave P, Taddei K, Sohrabi HR, Zetterberg H, Blennow K, Teunissen CE, Vanderstichele HM, Martins RN. Plasma glial fibrillary acidic protein is elevated in cognitively normal older adults at risk of Alzheimer's disease. Transl Psychiatry. 2021 Jan 11;11(1):27. PubMed.
Chatterjee P, Vermunt L, Gordon BA, Pedrini S, Boonkamp L, Armstrong NJ, Xiong C, Singh AK, Li Y, Sohrabi HR, Taddei K, Molloy M, Benzinger TL, Morris JC, Karch C, Berman S, Chhatwal J, Cruchaga C, Graff-Radford NR, Day GS, Farlow M, Fox N, Goate A, Hassenstab J, Lee JH, Levin J, McDade E, Mori H, Perrin R, Sanchez-Valle R, Schofield PR, Levey A, Jucker M, Masters CL, Fagan AM, Bateman RJ, Martins RN, Teunissen C, and the Dominantly Inherited Alzheimer Network. Plasma glial fibrillary acidic protein in autosomal dominant Alzheimer's disease: Associations with Aβ-PET, neurodegeneration, and cognition. Alzheimers Dement. 2022 Dec 28; PubMed.
Karolinska Institutet
Bellaver et al. are to be congratulated on this very interesting paper linking together Aβ and tau pathology with reactive astrogliosis as an important upstream event in the pathological cascade of AD. The high reactive astrogliosis in preclinical AD measured by GFAP in this study is in agreement with our earlier observations of high reactive astrogliosis measured by 11C-deprenyl PET in presymptomatic autosomal-dominant AD mutation (ADAD) carriers (Rodriguez-Vieitez et al., 2016), although the peak values of high 11C-deprenyl PET binding seem to occur earlier (17 years before estimated clinical symptoms) in comparison to the start of the increase in plasma GFAP levels (10 years before estimated symptoms) in ADAD carriers (Chatterjee et al., 2022; Johansson et al., 2023). 11C-deprenyl microPET studies have also demonstrated high astrogliosis preceding amyloid plaque deposition in AD APPswe transgenic mice (Rodriguez-Veitiez et al., 2015).
It is now important to further understand whether plasma GFAP reflects brain astrogliosis, or if plasma GFAP represents a different stage or form of astrocytes than in brain? It might be possible that plasma GFAP solely reflects an intermediate toxic astrocytic form but shows a strong correlation with Aβ positivity and plasma p-tau levels as demonstrated in this paper by Bellaver et al. Studies exploring new early astrocyte biomarkers should be encouraged, as for example the astrocytic α7 nicotinic acetylcholine receptors (Fontana et al., 2023).
References:
Rodriguez-Vieitez E, Saint-Aubert L, Carter SF, Almkvist O, Farid K, Schöll M, Chiotis K, Thordardottir S, Graff C, Wall A, Långström B, Nordberg A. Diverging longitudinal changes in astrocytosis and amyloid PET in autosomal dominant Alzheimer's disease. Brain. 2016 Mar;139(Pt 3):922-36. Epub 2016 Jan 26 PubMed.
Chatterjee D, Jacob RS, Ray S, Navalkar A, Singh N, Sengupta S, Gadhe L, Kadu P, Datta D, Paul A, Arunima S, Mehra S, Pindi C, Kumar S, Singru P, Senapati S, Maji SK. Co-aggregation and secondary nucleation in the life cycle of human prolactin/galanin functional amyloids. Elife. 2022 Mar 8;11 PubMed.
Johansson C, Thordardottir S, Laffita-Mesa J, Rodriguez-Vieitez E, Zetterberg H, Blennow K, Graff C. Plasma biomarker profiles in autosomal dominant Alzheimer's disease. Brain. 2023 Mar 1;146(3):1132-1140. PubMed.
Rodriguez-Vieitez E, Ni R, Gulyás B, Tóth M, Häggkvist J, Halldin C, Voytenko L, Marutle A, Nordberg A. Astrocytosis precedes amyloid plaque deposition in Alzheimer APPswe transgenic mouse brain: a correlative positron emission tomography and in vitro imaging study. Eur J Nucl Med Mol Imaging. 2015 Jun;42(7):1119-32. Epub 2015 Apr 17 PubMed.
Fontana IC, Kumar A, Nordberg A. The role of astrocytic α7 nicotinic acetylcholine receptors in Alzheimer disease. Nat Rev Neurol. 2023 May;19(5):278-288. Epub 2023 Mar 28 PubMed.
Cliniques Universitaires Saint-Luc and Massachusetts General Hospital
Université Catholique de Louvain
This important study addresses the puzzling observation that some clinically normal individuals with Aβ pathology do not demonstrate cognitive decline during many years, whereas others rapidly progress to cognitive impairment and dementia. Previous research had observed that tau pathology was more closely associated with cognition than amyloid, but clinical observations supporting a mechanistic explanation relating amyloid to tau pathology and cognition were missing so far. Here, Bruna Bellaver and colleagues convincingly demonstrate, in a very large, multi-cohorts analysis, that tau pathology (as observed with plasma or PET) is only observed in high-amyloid individuals with astrocyte activation.
These results shed light on an underexplored mechanism linking amyloid and tau: astrocyte activation, and more broadly, neuroinflammation. Providing such a mechanism linking amyloid and tau is key for early clinical interventions. First, because it allows better targeting individuals who will progress in the next few years; second, because it provides new research avenues to target AD: astrocytes modulators.
The use of longitudinal tau measures provides evidence that tau accumulation is a downstream event compared to amyloid and astrocyte activation. However, it is not clear whether astrocyte activation precedes, follows, or develops independently of amyloid accumulation.
Beyond the present results, this study raises the question about the role of neuroinflammation, a process common to many neurological disorders (multiple sclerosis, traumatic brain injury, epilepsy, infections, or tumors of the central nervous system) in the development of Alzheimer's pathology. Patients with such medical history are most often excluded from AD clinical research; however, they often complain about cognitive impairment. Exploring the accumulation of amyloid and tau pathology in patients with other neurological conditions would be of utmost interest to better understand the onset of cognitive impairment in these patients.
Make a Comment
To make a comment you must login or register.