High-Dose Gantenerumab Lowers Plaque Load
Quick Links
At this year’s Clinical Trials on Amyloid Disease meeting, held November 1–4 in Boston, Roche scientists showed that high doses of gantenerumab reduced amyloid plaques in the brains of people with Alzheimer’s disease, and that raising the dose slowly mitigated the risk of side effects. Results from the ongoing open-label extensions (OLE) of two Phase 3 trials indicated that monthly injections under the skin of 900 mg and 1,200 mg gantenerumab reduced brain amyloid by up to 15 percent over six to nine months. For one-third of treated patients, uptake of the amyloid PET ligand florbetapir dropped below a predetermined threshold for positivity. Researchers at the meeting said the data were encouraging, though they cautioned that the number of patients was small and interpretation tricky because participants received different doses of drug for different periods of time.
- Gradually upping the dose of gantenerumab reduces risk of ARIA.
- In open-label extension, highest dose lowered brain amyloid.
- High dose predicted to eliminate a quarter of amyloid over two years.
“I am highly optimistic about the late-onset sporadic AD data from the OLE PET study, which clearly demonstrated a biologically significant decrease in amyloid over six to nine months. This demonstrates that one of the main pathologies of AD can be reversed with gantenerumab,” said Randy Bateman of Washington University, St. Louis.
The various dosing regimens came from a need to reduce the risk of amyloid-related imaging abnormalities (ARIA), namely vasogenic edema (ARIA-E) and micro-hemorrhages (ARIA-H). The former in particular is a common side effect of amyloid immunotherapy. At CTAD, Rachelle Doody, who left Baylor to join F. Hoffmann-La Roche, Basel, Switzerland, outlined the rationale for the OLE protocols for the Scarlet RoAD and Marguerite RoAD trials, neither of which had shown efficacy on primary endpoints (Dec 2014 news). Pharmacokinetic and pharmacodynamic analysis from the halted Scarlet RoAD trial suggested that, even though the trial was negative on the primary endpoint, participants who had had the highest gantenerumab exposure, and those in whom disease progressed fast, did appear to benefit both in amyloid reduction and ADAS-cog, respectively (Nov 2015 conference news).
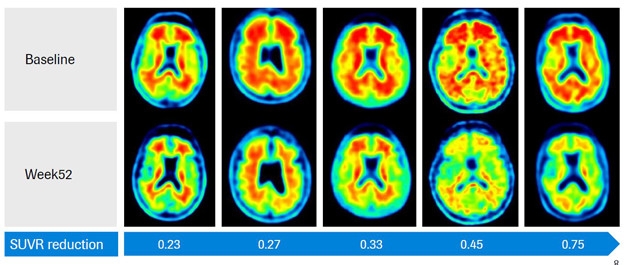
Amyloid Cleared? Five patients titrated up to high-dose gantenerumab saw a reduction in florbetapir SUVR of up to 0.75. [Courtesy of Gregory Klein, F. Hoffmann-La Roche.]
A model built with data from Scarlet RoAD and with published data on another therapeutic antibody, Biogen’s aducanumab, predicted that amyloid would need to be reduced in the brain by at least 20 percent to see a slowing of cognitive decline, said Doody. The 105 mg and 225 mg doses used in Scarlet RoAD would not cut it. Instead, the model predicted that 1,200 mg of gantenerumab subcutaneously would be needed over a two-year period. Indeed, the DIAN-TU trial of gantenerumab in people with autosomal-dominant AD mutations increased the dose subsequent to this analysis.
The problem at high doses would be ARIA. Roche scientists then modeled gantenerumab’s likely effect on ARIA, taking into account dose, duration of treatment, and ApoE genotype—a known risk for ARIA. That model informed the dosing regimen in the open-label extension studies. Patients who wished to continue treatment would eventually receive the 1,200 mg dose, but would be titrated up based on their prior exposure to the drug and their ApoE4 status. Hence, patients started on either 105, 225, 300, 450, or 600 mg doses, and got higher doses every two months until they had reached 1,200 mg. Some patients ended up on the high dose for 10 months, others for only two, all while being monitored for ARIA by way of MRI scans. If patients experienced significant ARIA, they paused treatment until it resolved.
Doody said that the titration reduced ARIA-E as expected. The model predicted that most ARIA-E would occur during the first few months, then taper off even as the dose went up further, and that is what happened. At CTAD, Doody showed closely overlapping plots of predicted versus recorded ARIA-E over time.
Mirjana Andjelkovic, also from Roche, offered details in a talk and a poster. Out of 228 patients who enrolled in the Marguerite RoAD OLE, 203 had at least one MRI post-baseline and 58 of them had ARIA-E. For most, it was asymptomatic. Fourteen people had a mild headache or confusion; three developed more serious symptoms, two having a seizure that resolved, and one a possible stroke.
Roche used two titration protocols—one reaching the target dose of 1,200 after six months, the other after 10 months. Because Scarlet RoAD participants were taken off gantenerumab for more than a year before the open-label extension started, their Alzheimer’s had progressed. Even so, Andjelkovic said, overall safety findings were unchanged on the higher dose.
Patients who were titrated up more slowly had less ARIA-E. For example, among ApoE4 carriers who eventually received 1,200 mg, 16 percent developed ARIA-E if started on 225 mg as compared to 30 percent of those who started on 400 mg. Similarly, the incidence among ApoE4 noncarriers who started on 600 mg was double that among those starting on 300 mg.
Of the patients who experienced ARIA-E, 35 also had signs of ARIA-H, as did 15 patients who tested negative for ARIA-E. Clinicians generally consider ARIA-H less of a concern, and Doody noted that it crops up in placebo groups as well. In summary, Doody felt that higher doses of gantenerumab could be used safely. “I think it is possible we can optimize the schedule to reduce ARIA and to use the same titration for both ApoE4 carriers and noncarriers, which would make trials more manageable,” Doody said.
What about amyloid reduction? At CTAD, Gregory Klein, also from Roche, showed the first data from an 81-patient PET sub-study of the OLE trials. Klein focused on patients deemed to have sufficient antibody that it might move amyloid from the brain, i.e., people who had received at least six doses of 900 mg or 1,200 mg during the OLE period. Forty patients fit the bill so far. Klein subdivided them into three bins: nine patients who had continued from Scarlet RoAD; 14 from the original Marguerite RoAD placebo group; and 17 who had been in that trial’s treatment group. The distinctions matter because these patients started out with different levels of amyloid and had different exposures to high-dose gantenerumab in the OLEs. Scarlet RoAD enrolled people with prodromal AD, whose baseline florbetapir standard-uptake value ratio (SUVR) in the OLE rang in at 1.45. Marguerite RoAD enrolled people with mild AD, which was reflected in higher baseline OLE SUVRs of 1.79 and 1.7, for those in the original control and treatment groups, respectively. Further, Scarlet RoAD participants had, on average, 5.7 months of high-dose immunotherapy in the OLE, whereas for those from the Marguerite RoAD control and treatment arms it was 6.8 and 9.4 months.
Klein showed that SUVRs for the nine Scarlet RoAD patients fell by 0.13, or 9 percent. The drop doubled in the Marguerite RoAD groups to 0.24 and 0.27, or about 15 percent. Klein said this fit with Roche’s model, which had predicted a 26 percent reduction in amyloid over 20 months of high-dose treatment. For one-third of the patients the SUVR had dropped below the predetermined cutoff for amyloid positivity. At 1.4, the cutoff is higher than typically used in the field. It was determined ad hoc by comparing uptake from six cortical regions and normalizing to the cerebellum. Klein noted that absolute SUVRs are not comparable between methodologies.
Researchers at CTAD found Klein’s data promising, but asked about effects on cognition. Do people with more amyloid removal decline less? Klein replied that because it has no placebo group and few participants, the OLE is not powered to answer this question, though as participants are continuing on treatment they are being assessed for cognition.
Others wondered what might happen when treatment ends. Will brain amyloid return? Researchers are studying this question. “We will have two-year scan data, and we are conducting retrospective analyses of earlier studies to see what happens when dosing stops,” Klein said.
Roche is planning two new Phase 3 clinical trials, called GRADUATE 1 and 2. According to a company spokesperson, starting in early 2018 each trial will enroll 750 people with prodromal to mild AD, and treat them for two years with subcutaneous injections of antibody or placebo. Roche did not disclose the dose except to say it will be higher than in the previous trials, and the trials will employ a single titration scheme for both ApoE4 carriers and noncarriers.
The gantenerumab findings are in sync with CTAD presentations on the anti-Aβ antibody aducanumab. Biogen researchers showed marked amyloid reduction on the highest dose with long-term exposure, and mitigation of ARIA with a dose titration protocol (see Part 1 of this series).—Tom Fagan
References
Therapeutics Citations
News Citations
- End of the RoAD for Gantenerumab? Roche Declares Prodromal Alzheimer’s Trial Futile
- Gantenerumab, Aducanumab: Bobbing Up and Down While Navigating Currents of Trial Design
- 10th CTAD: Finally, Alzheimer’s Field Is Serious About Prevention Trials
External Citations
Further Reading
No Available Further Reading
Annotate
To make an annotation you must Login or Register.
Comments
No Available Comments
Make a Comment
To make a comment you must login or register.