The Alzheimer's Disease Neuroimaging Initiative is the most expensive AD study the NIH has ever funded. Expectations are that it will speak with the authoritative voice of a 58-center, three-year observation of 819 research participants above a current cacophony of smaller voices touting the results of their single-center studies.
ADNI has broken ground in standardizing the exact ways in which all those centers gather data across a broad range of assessments—clinical, psychometric, imaging, biochemical—in these volunteers. It has broken ground in making those data sets freely and easily available to every scientist worldwide for analysis. It has broken ground as a pre-competitive, public-private partnership, and has inspired similar efforts around the globe. ADNI aspires to provide the data that could make it possible to predict who will get AD and how quickly they will get it, and to invite people at earlier stages, even presymptomatically eventually, into biomarker-driven therapeutic trials.
As ADNI Turns Four, $64 Million Data Start Rolling In
The Alzheimer Disease Neuroimaging Initiative (ADNI) is the largest AD study the National Institutes of Health have ever funded. Announced in October 2004 and set to run until 2010, this public-private consortium has engaged 59 research centers in the U.S. and Canada in a massive effort to follow 821 research volunteers for three years. The year 2005 went by preparing sites, building informatics tools, and enrolling the first patients, 2006 and 2007 were spent enrolling and seeing patients, and now in 2008 waves of data have begun flooding in. In terms of data gathering, the study is nearing its midway point. In terms of analysis, it is only scratching the surface of what is yet to come; hence, drawing major conclusions would be premature. Still, the beginning of ADNI’s final year is a good moment in time to take its pulse and peek at the preliminary scientific trends that are beginning to emerge.
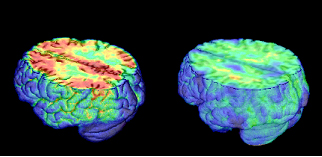
Surface Rendering of a Shrunken Cortex in Alzheimer Disease.Image credit: Laboratory of Neuro Imaging (LONI), UCLA
As of now, seven papers on ADNI results have been published, two dozen manuscripts are submitted, some 60 abstracts dealing directly or indirectly with ADNI were presented at the recent International Conference on Alzheimer’s Disease (ICAD) last July in Chicago, and 300 investigators from across the world have downloaded ADNI data for their own analysis. Add-on studies for genetics and amyloid imaging are plugging along; neuropathology validation is set up and awaiting cases. ADNI has built on the clinical infrastructure established previously by the Alzheimer’s Disease Cooperative Study (ADCS). Pharmaceutical companies developing AD drugs have implemented ADNI methodologies in their newer clinical trials. Early data are confirming the main findings of many prior, much smaller imaging and biomarker studies. Early statistical calculations are already hinting that CSF and imaging markers have more power than clinical methods to measure disease progression. Baseline results on the normal control subjects indicate that some of them might have preclinical AD; these data warrant close observation of this population for years to come. ADNI scientists are beginning to plan for a hoped-for expansion, aka ADNI2. Finally, ADNI has caught on around the world, with similar efforts underway in Australia, Japan, Europe, and China. For more on each of these points, read our ADNI 2008 series.
This website has covered the motivation behind ADNI and its major purpose when the study started (see ARF related news story). ADNI itself has an informational website that offers a wealth of freely downloadable slide presentations, protocols, and other materials on ADNI’s organizational structure, goals, and related activities. In brief, ADNI is a longitudinal, observational study that tracks how various measures of structural, functional, and amyloid imaging, as well as fluid biomarkers, change over time in people who enter the study either cognitively normal or with a diagnosis of mild cognitive impairment (MCI), or AD. ADNI compares a host of candidate imaging analyses and biomarkers side-by-side in the same study population, and will relate each marker’s change over time to show how that person’s cognitive and clinical stage also changed over the same period. This can move the field past its current stage, where single-center studies tend to use different ways of acquiring and analyzing data on different candidate biomarkers in different, smaller sets of people. “The literature is full of reports of the value or technique X or method Y in tracking progression or in diagnosis; however, it is difficult to compare reports because the subject groups are always different,” Nick Fox wrote to ARF. Fox is at University College London, the only non-U.S. ADNI preparation and analysis center. ADNI aspires to help the field anoint consensus biomarkers that the pharmaceutical industry and ADCS will incorporate into their therapeutic trials. The goal is that drug trials will eventually treat validated biomarkers of AD instead of treating cognition with its noisy outcome measures. That would cut the cost and length of drug trials and make prevention trials of presymptomatic AD practical (see ARF related news story).
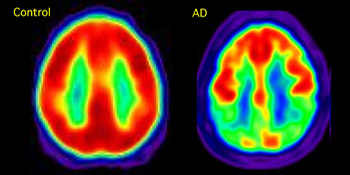
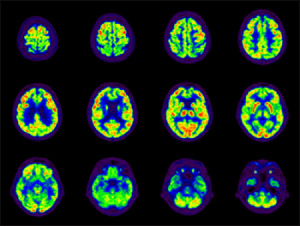
A Composite Picture of Glucose Metabolism Using PET and the Tracer FDG
The AD patient on the right shows reduced glucose metabolism in temporoparietal cortex, a hallmark of the disease and a potential biomarker that is being explored in ADNI. Image credit: William Jagust
Inspiration for ADNI Neil Buckholtz, who heads the Dementias of Aging program at the National Institute on Aging (NIA), is widely credited with spearheading support for ADNI by bringing different stakeholders together. In discussions with researchers from pharmaceutical companies as early as the mid-1990s, one problem was even then that the companies wanted to develop disease-modifying drugs for AD but had no guidelines from the FDA on how to show if such drugs worked. “We thought it would be useful to serve as a broker between pharmaceutical companies and academic scientists to develop the best instruments and methodologies to measure change over time, so that companies could later test if their drug modifies that progression,” Buckholtz recalled. Because this goal addressed a problem that bedevils all drug makers in the field, it fell into what is called “precompetitive space.” This buzzword denotes areas of common ground where companies that compete fiercely around their products can invest jointly, and even collaborate closely, to generate a set of data that is open to every player in the field. “The ability to standardize imaging approaches, to identify patients early in disease, and to monitor treatment with disease progression markers are hurdles shared across pharma, and ADNI has provided solutions to some of industry’s more intractable problems,” commented Holly Soares of Pfizer, a member of ADNI’s industry advisory board.
To build a public-private consortium, Buckholtz engaged the Foundation for the National Institutes of Health, which was set up by Congress to be able to solicit funds from private groups (the NIA itself cannot do that). The Foundation for the NIH raised money from more than a dozen pharma companies as well as the Alzheimer’s Association and the Alzheimer’s Disease Discovery Foundation (see also ADNI Sponsors), and transferred it to the NIA. The institute used it to fund a grant submitted by Michael Weiner of the University of California, San Francisco, ADNI’s principal investigator. Forty million dollars of that grant came from NIH, and about $24 million through the Foundation of the NIH. By summer 2008, the number of companies in the private consortium had grown to 15. It has supported extensions and add-on studies (see Part 5 of this series, and below). Foundation staff has helped identify industry partners for ADNI and organized a symposium to support communication between the ADNI consortium and regulatory agencies.
ADNI’s industry sponsors each dispatch a representative to an advisory board that supports the overall study, and they also have liaisons to individual ADNI cores, i.e., the scanner manufacturers to the imaging core, the bioassay company to the biomarker core, pharma companies to the clinical core, etc. Dubbed ISAB, this board lends its expertise to the design and execution of ADNI and its add-on studies. Their work is more than nominal. They meet once a month by phone and twice a year in person. For example, the board helped with developing best practices, guidelines, and standard operating procedures—the nitty-gritty stuff that is often boring to the academic investigator but that can sink multicenter studies. Moreover, the ISAB played a role in expanding the CSF component of ADNI from its original target of one fifth of participants to more than half of participants. It helped the clinical sites do that by developing short videos based on prior data Elaine Peskind at University of Washington, Seattle, had generated. Those videos on the one hand featured use of a smaller needle and generally trained clinical staff to conduct standardized lumbar punctures well, and on the other offered education that helped dispel misconceptions about lumbar puncture among volunteers. The private consortium then funded an ongoing extension of the original CSF study, which had planned to collect baseline and year 1 time points, to collect year 2 and 3 samples, as well. “The partnership has worked very well,” Buckholtz said. “The industry partners provide intellectual input. They do not push ADNI to their individual advantage.”
Importantly, ADNI data are open and freely accessible to a degree that is unprecedented in AD research. The study has an informatics core headed by Art Toga of the University of California, Los Angeles. Part of Toga’s charge was to build systems that make it possible for all 59 participating ADNI centers to upload their data to UCLA’s Laboratory of Neuro Imaging, and likewise, for any external scientist around the world who wants to analyze ADNI data to download it from the LONI site. ADNI’s clinical and neuropsychology data are available there, as well as its biomarker and imaging data. More than 32,000 MR and PET scans currently are on this site, and some 300 investigators have downloaded 340,000 images already, Weiner said during a lecture at ICAD. In addition, genetic data will be uploaded this October, according to Andrew Saykin of Indiana University School of Medicine, Indianapolis, who heads the genetics add-on studies, and some imaging data from the Australian AIBL study will follow in early 2009 (see Part 6 of this series).
ADNI is the first Alzheimer’s research study where scientists sitting at their computer anywhere in the world can obtain the data, analyze it, and then publish their results, without having to see a patient or tapping into a clinical system. “It is very easy to do a query and download images and associated cognitive and lab data,” wrote Sterling Johnson of the University of Wisconsin. “This accessibility reflects a shift in the way scientists think about the boundaries of data ownership. It also reflects the urgency we all feel about the growing problem of AD as the population ages, and the lack of effective interventions.” Beyond data, biofluids can be made available to non-ADNI scientists, as well. This access is tightly managed, however, because the fluids are precious and limited. ADNI’s resource allocation review committee welcomes requests, and assesses each individually.—Gabrielle Strobel.
This is Part 1 of a six-part series. See also Parts 2, 3, 4, 5, 6. Read the entire series [.pdf].
ADNI Results: A Story of Standardization and Science
The results of ADNI are arriving at two different levels. One is the aspect of coordinating and standardizing multisite procedures (the “how”); the other is actual new scientific data (the “what”). On the “how,” the verdict from numerous scientists interviewed for this series was that ADNI has set the standard for future multisite brain imaging studies. Cliff Jack at the Mayo Clinic in Rochester, Minnesota, directed standardization of the MRI imaging. This project required rewriting scanning pulse sequences for three major MRI vendors and persuading the vendors to have these sequences installed, as well as use and testing of a geometric phantom for calibration. His group also provides quality control for every uploaded ADNI MRI scan. “The MRI analyses are state of the art, providing regional maps of involvement that may be useful for patient selection or measuring progression,” comments Michael Grundman of Elan Pharmaceuticals in South San Francisco.
Likewise, Robert Koeppe at the University of Michigan in Ann Arbor, and Bill Jagust at the University of California, Berkeley, normalized and performed quality control on the FDG-PET data collected on a variety of different PET scanners at more than 50 sites. This work, in turn, laid the groundwork for the subsequent PIB-PET ADNI substudy (see Part 5 of this series) to do the same. For their part, Leslie Shaw and John Trojanowski at the University of Pennsylvania Medical School in Philadelphia lead a qualification study on CSF biomarkers in which seven expert labs—some academic, some industrial—in four different countries showed that ADNI’s multiplex assay for Aβ and tau measurements were reproducible day in and day out within less than 10 percent variability. This strengthened the validity of the fluid measurements across ADNI.
“ADNI has succeeded beyond expectations in terms of delivering initial data in time for some critical studies, as well as advancing the standards for multisite MRI, FDG-PET, and 11C PIB studies, not to mention clinical trial quality assays for important analytes in cerebrospinal fluid,” noted Bill Potter, who represents Merck on ADNI’s Industry Scientific Advisory Board. “Simply working out what it takes to obtain quality data across sites for all of these modalities has been worth the investment for any company planning to do studies of compounds that might modify the course of AD.” Sources interviewed for this article generally confirmed that both the ADCS and pharmaceutical companies are using ADNI’s methodologies in ongoing clinical trials.
On the “what,” i.e., the research data, it is early days. The comprehensive comparison of methods is not possible for another year. With the first year of follow-up complete, ADNI scientists are currently analyzing the fluid specimens and summarizing the raw imaging data computationally. Laurel Beckett at University of California, Davis, heads ADNI’s statistics core. “We are really trying to set up for the big push to summarize our first year of very complex multifactorial tracking of change.” At the International Conference on Alzheimer’s Disease (ICAD), held last July in Chicago, the loudest buzz surrounded the three issues of confirming previous work, power calculations for trials, and intriguing signals in the normal controls of ADNI. Here are highlights of the preliminary analysis of the available data so far.
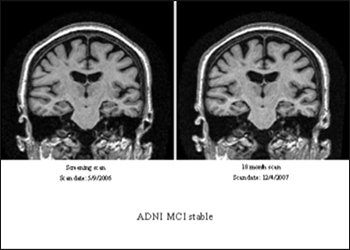
ADNI has completed enrollment of 819 people, 229 normal, 398 MCI, 192 AD. In the two years since their first assessment, 26 percent of those with MCI progressed to a diagnosis of AD, while less than 5 percent of the normal controls developed MCI. An even smaller fraction reverted back to MCI from AD and to normal status from MCI. These conversions will be critical to validate how clinically relevant the imaging and biomarker changes are that ADNI is beginning to show. ADNI scientists showed the results of the complete one-year follow-up of the participant’s clinical and neuropsychological and MRI data in the form of spaghetti plots. These are colorful overlaid line graphs showing how each person fared over time on a given measure. They show at a glance that the data confirm overall expectations. That is, clinical measures show expected trends in normal control, MCI, and AD, but do so with a lot of zigzagging, whereas imaging data show the expected trends with much less fluctuation. The MCI group is the most heterogeneous at this point.
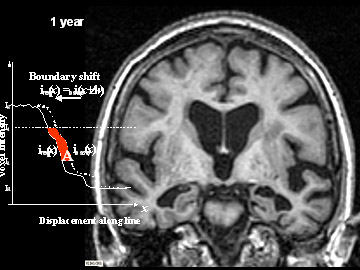
A handful of different laboratories within the MRI core (and many more outside of it) are each conducting their own analyses of the same magnetic resonance scans. For example, Nick Fox’s group at University College, London, measures boundary shift integrals, Norbert Schuff’s at University of California, San Francisco, focuses on hippocampal volume, Colin Studholmen’s at UCSF and Paul Thompson’s at UCLA use tensor-based analysis, Gene Alexander’s at the University of Arizona tests vowel-based morphometry, and Anders Dale’s at UCSD uses an automated surface reconstruction software called Freesurfer. All these are different approaches to quantify how the brain’s tissue shrinks and its ventricles expand over time. The goal is to find robust measures of change that reflect more than merely a person’s advancing age but indeed correlate tightly with how a person’s clinical state worsens over time. It is too early to draw a definitive comparison because much of the longitudinal data is yet to come. That said, early ADNI data confirm previous findings from smaller studies that certain brain areas, especially in the hippocampus, atrophy early in AD and offer a robust marker for change. Moreover, it appears as if hippocampal volume loss accelerates as the disease progresses clinically, Michael Weiner of UCSF noted at ICAD (see also Nestor et al., 2008). It will be interesting to see if this correlates also with a biomarker change.
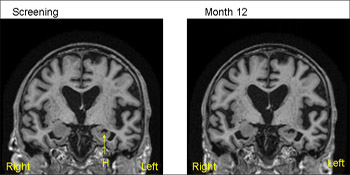
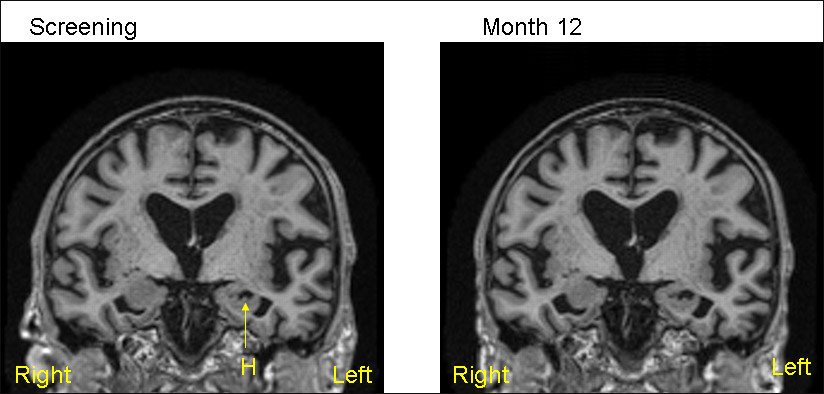
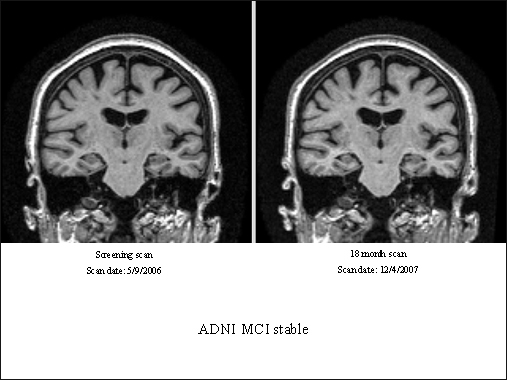
1.5T MRI scans from the same patient (MCI) from ADNI—baseline (screening) on the left and 12 months on the right. The 12-month scan has been registered to the baseline so that both scans are positional matched (the same position and orientation) so that comparisons are facilitated. Note that even with simple visual inspection one can see loss of volume of the hippocampus (H) with increase in the CSF filled space (temporal horn) around the hippocampus. View larger image. Image credit: Nick Fox
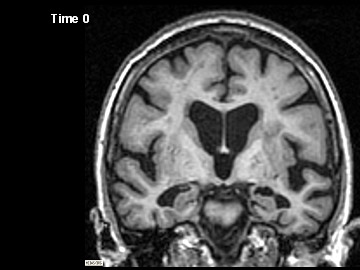
ADNI Participant With AD Imaged at Study Entry and One Year Later
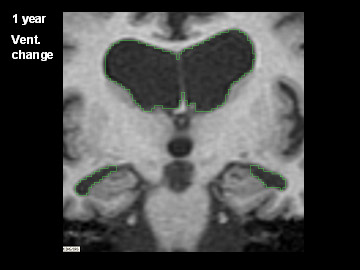
Flicking back and forth between image 1 and 2 illustrates how the boundaries of the gray matter in the person's brain have shifted (i.e., shrunk). The red area quantifies the volume loss during this year. Images 3 and 4 illustrate the corresponding expansion of the fluid-filled ventricles in the same person during this time. Image credit: Nick Fox, University College London
Findings like this are where the ADNI biostatisticians come in to make sure that ways of understanding how imaging data relate to clinical change are robust in the face of how the real data behave, Beckett explained. “For example, if we had assumed that hippocampal volume shrinks at a steady pace in AD, but found that in fact the rate accelerated over the course of our follow-up, we’d have to rethink how to relate that to, say, change in the ADAS-Cog or other measures of cognitive function.”
Likewise, functional imaging data using FDG-PET (which indicates glucose use in brain areas) are undergoing different types of analyses to see which provide the best markers. Jagust, Norman Foster at the University of Utah, Salt Lake City, and Eric Reiman at the University of Arizona, Phoenix, are leading these groups. One odd finding by Foster’s group stood out right away, Weiner noted at ICAD, namely that one in 10 AD cases appeared to have a more FTD-like than AD-like pattern of brain metabolism, suggesting that some fraction of ADNI's AD patients may at autopsy prove to have been misdiagnosed. Headed by Nigel Cairns, ADNI's neuropathology core at Washington University in St. Louis, Missouri, provides the gold standard diagnosis for ADNI participants who die after entering the study. Indeed, Cairns and his colleagues Lisa Taylor-Reinwald have already determined that, of the three brains that have come to autopsy from ADNI participants, the first had major Lewy body pathology besides classic AD pathology even though the person had been clinically diagnosed with AD, not DLB. Hence the definitive diagnosis partly disagreed with the clinical assessment. This reinforces the notion that an inherent error rate in the clinical diagnosis in effect puts a “glass ceiling” on the success rate of predictive tests, which are typically measured against the clinical diagnosis.
That aside, the overall preliminary finding of the FDG-PET analyses are that reduced metabolism in the parietal/temporal lobe marks progression. Emerging data from Reiman’s and Jagust’s groups indicate that unbiased analyses tend to beat assumptions made on previously specified anatomical regions of interest in finding the earliest and strongest FDG-PET changes. These analyses point to the posterior cingulate and the precuneus as brain areas that are the first to be on the wane. Overall, the most precise MRI measures appear to trump FDG-PET measures at this point, and scanning people in the higher field strength 3.0 T magnets did not appear to improve data significantly over those gleaned in the standard 1.5 T scanners. Check Part 3 of this series for more ADNI results.—Gabrielle Strobel.
This is Part 2 of a six-part series. See also Parts 1, 3, 4, 5, 6. Read the entire series [.pdf].
One goal of ADNI is to make clinical trials sharper. To that end, scientists are running power calculations for hypothetical trials. In essence, they play a “what if” game to see by how much inclusion of a given biomarker or type of imaging would reduce the number of participants needed in each arm of a trial of a disease-modifying drug, for example, a trial designed to detect a 25 percent slowing of cognitive decline. These estimates, in turn, use calculations of how many people need to be in each arm to detect a corresponding change in the given biomarker/imaging modality. At present, these exercises are using data from repeat scans at baseline and year 1. ADNI’s lead biostatistician Laurel Beckett of the University of California, Davis, explains: “This is one way of putting the different measures on the same scale. If you believe that change in the measurement is bad clinically, and you have a treatment that will slow it down, how large a study do you have to do to provide persuasive evidence that it works? The 25 percent reduction is arbitrary; we could have chosen 33 or 50 percent. The larger the reduction we think we can get, the smaller the study we need. It's a lot easier to spot huge effects than modest ones. But it's also easier to spot effects if you have very stable, steady change, rather than up-and-down, noisy, good-day, bad-day sort of paths. So this analysis basically asks: how strong is the “signal” for change compared to the “noise,” but measures the strength of the signal by how easy it would be to detect a change in the signal.”
Consider this example. Using the ADAS-Cog, a 25 percent trial would need 467 people with AD, or 1,982 people with MCI per group. Using the CDR sum of boxes, those numbers drop to 424 AD patients and 764 with MCI. However, detecting 25 percent change in certain MRI measures (such as Freesurfer, boundary shift integral, or certain white matter changes) would only require some 50 to 100 AD cases or about 100 to 150 MCI cases per group. In functional imaging so far, only an analysis performed by the Arizona group appears to slash sample size significantly (160 per group in AD, 626 for MCI), scientists reported at the International Conference on Alzheimer’s Disease (ICAD) last July in Chicago. “We already see that imaging methods have much more statistical power than clinical methods to measure change,” Michael Weiner of University of California, San Francisco, wrote to ARF.
FDG-PET scan of an ADNI participant with mild cognitive impairment. Image credit: ADNI PET Core
And it’s not just imaging. Also at ICAD, Mike Donohue, a biostatistician at UC San Diego, presented a similar exercise where he used the publicly available ADNI data to see if incorporating its measures as baseline covariates would increase the power of a trial geared toward detecting a 30 percent dent in ADAS-Cog worsening. Donohue reported that the needed group sizes would be significantly smaller if the trials included baseline measurement of the volume of the temporal lobe or the hippocampus, or the CSF tau/Aβ42 ratio. Even outside of ADNI, power calculations are catching on. Also at ICAD, in the last hour of the conference, David Holtzman of Washington University in St. Louis, Missouri, updated the audience on his center’s ongoing studies combining CSF biomarkers and imaging to predict rates of clinical decline in cognitively normal or very mildly impaired people (see below). In the course of this talk, Holtzman noted that the WashU data support calculations, whereby prevention trials powered to detect a 50 percent effect size would need only half as many participants per arm if they selected people by their low CSF 42 values versus merely enrolling people with the lowest detectable clinical dementia rating (CDR of 0.5).
Spinal Fluid Spills Its Secrets
ADNI’s biomarker effort is the largest biofluids study done in AD so far. It is collecting CSF at baseline, year 1, 2, and 3 in a subset of participants. (It is also collecting plasma and urine, but their analysis is less advanced.) At this point, the biomarker core lab has uploaded to the LONI baseline data on all 416 participants, that is, their CSF Aβ42, tau, phospho-tau concentrations, and the tau/Aβ ratio. The 56 ADNI sites that are performing lumbar punctures are presently collecting year 2 samples, while the biomarker core scientists are analyzing year 1 data and the few year 2 measurements that have already come in, said Leslie Shaw of the University of Pennsylvania Medical School in Philadelphia, who co-directs ADNI’s biomarker core together with John Trojanowski. Already available at this point, from interviews, ICAD presentations, and slide presentations at adni-info.org, are the results of the baseline data compared with people’s diagnoses, and with information of whose diagnosis has changed since baseline.
This analysis first established cutoffs for normal versus pathological values in the markers by running the ADNI assay in a separate UPenn cohort of autopsy-controlled cases who had donated CSF samples prior to death. Using those cutoffs in the ADNI sample, the scientists then showed that of all CSF markers tested, CSF Aβ42 best characterized the groups. Moreover, of the 37 ADNI participants to date who had entered the study with an MCI diagnosis but had progressed to AD by year 1, 34 at baseline had a pathological CSF signature of low Aβ42/high tau and phospho-tau. This signature, then, would appear to predict conversion from MCI to AD and may help sort participants of future MCI trials. About three quarters of people in the baseline MCI group had this signature. Overall, the ADNI CSF study appears to support what smaller studies have shown before (e.g., Hansson et al., 2006). “The findings have confirmed and extended data that suggested measures of brain volume, amyloid load, and CSF biochemistry may be combined to sort those subjects with extremely mild symptoms (MCI) who will progress to full symptomatic AD within a relatively brief time (one to two years) from those who will show no clinical deterioration,” commented William Potter of Merck Research Laboratories.
The second insight that raised eyebrows is that up to half of the 229 normal controls enrolled in ADNI might not be aging so normally. Instead, the data suggest “that some of them have signals of early, preclinical AD,” Weiner wrote to ARF. Shaw agreed: “The group that many of us have been considering as true controls in the sense of comparing disease versus non-disease is probably not a true control.” This sense emerged from a first peek at several related datasets. For one, Beckett presented at ICAD that while the normal subjects overall had no clinical/neuropsychological changes between baseline and year 1, their brains were changing subtly. Many of them had noticeable brain atrophy, hippocampal atrophy, and ventricular enlargement. Intriguingly, the brain shrinkage correlated with the biochemistry in that those people who fell into the lowest quartile of CSF Aβ42 concentration at baseline also had the fastest changes. These folks were not older than the other normal controls, but they did have more ApoE4 carriers among them.
ADNI has no data yet to say whether this is aging or foreshadows cognitive decline; smaller studies at individual institutions, for example, WashU, would suggest the latter. According to Chet Mathis at the University of Pittsburgh School of Medicine, who heads the amyloid imaging substudy, almost 50 percent of ADNI normal controls are PIB-positive. According to Shaw, some 40 percent of that group have a pathological biomarker signature (i.e., low CSF Aβ42/high tau). Here again, ADNI confirms prior results by Tom Montine and colleagues at University of Washington, Seattle, by Erik Stomrud and colleagues, and also by Anne Fagan and colleagues of Washington University, St. Louis, who have argued for some time that this CSF signature represents a biological red flag of future AD in cognitively normal elderly people (Li et al., 2007; Stomrud et al., 2007; Fagan et al., 2007). This ADNI result also confirms older neuropathological findings that up to 40 percent of cognitively normal people in their seventies have “preclinical” Alzheimer disease in their brain (e.g., Price and Morris, 1999).
MRI—CSF—amyloid imaging: are all these measures abnormal in the same people? In response to this question, Beckett wrote “The numbers here are small and we have not looked at all the associations yet, but at least in part, yes.” She cautioned that none of these data in normal controls can yet be tied to clinical change on ADAS-Cog or MMSE, though subtle changes might show up in certain highly sensitive tools, for example, timed performance tests. “Whatever is going on here, and it's very provocative, is all still under the radar from a clinical perspective.… This is, to my mind, one of the very most exciting parts—it's like reading the opening chapter of a gripping thriller, and then finding that it is ‘to be continued.’”
Future of ADNI
The next two episodes (year 2 and 3 data) will come before long. Beyond that lies a second season, in other words, ADNI2. Hopes for a continuation are high, though nobody knows if the funding for it will come through. At this point, ADNI investigators are thinking toward a grant submission in the fall of 2009 by discussing what shape ADNI2 could take. One priority many scientists expressed was to follow the current normal control and MCI groups past three years, and to enroll new normal controls in order to find out in which sequence predictive imaging and biomarkers changes appear in a still-healthy person. A related goal is to try to close the gap between true normal aging and MCI by identifying a more mildly impaired group or high-risk groups. Part of this can be done based on the results of ADNI, which already appear to define a presymptomatic stage characterized by a combination of risk factors, such as ApoE4, brain amyloid, pathologic CSF Aβ/tau, reduced FDG-PET signal in posterior cingulate, and shrinkage of the hippocampus.
An ADNI2 would include an 18F amyloid imaging from the start, though just how sensitive the 18F tracers are at picking up the very earliest signals in clinically normal people remains to be ascertained. Fluid biomarker and proteomic analyses would be expanded. ADNI2 would contain a genetics core to build on the work of the current ADNI genetics working group.
At ICAD, Weiner told the audience that ideas for ADNI2 are welcome, and that now is the time to formulate them. “Other areas worth exploring include additional cognitive batteries and functional instruments, or computerized batteries (see ARF related news story) suited for early patients, simplified screening tests that could be used by primary care practitioners, and measurement of peripheral markers that may indicate an AD phenotype or predict progression,” wrote Michael Grundman of Elan Pharmaceuticals in South San Francisco. For his part, Merck’s Potter added that the ISAB is working with colleagues in academia, at the NIA and FDA, to define the value of an ADNI2 effort to better understand how to identify early subjects, and that these issues will dominate a meeting later this month. “Coupled with this is an exploration of whether a regulatory path could be established for bringing forward a preventive treatment based on biomarkers, with a post-marketing requirement to establish definitive evidence that subjects are protected from emergence of symptomatic AD as currently diagnosed,” Potter wrote.—Gabrielle Strobel.
This is Part 3 of a six-part series. See also Parts 1, 2, 4, 5, 6. Read the entire series [.pdf].
Add to ADNI: Imaging Amyloid and Analyzing the Genome
Typically, a large investment in big science attracts ideas on how to get more bang for the buck once the original study is on its way. Likewise, ADNI evolved from its original design. For one, the original biomarker protocol changed when the investigators realized they had underestimated the participants’ willingness to undergo a lumbar puncture. More than half did, as opposed to the expected one-fifth. A privately funded extension now ensures that CSF biochemistry gets done not only for baseline and year 1, but also at year 2 and 3 visits. This completes the longitudinal dataset available for each person. Moreover, the same funders encouraged a biomarker qualification study to certify the performance of the CSF biomarker assay. That study subsequently established that the way the assay was performed actually yielded reproducible and reasonably identical results in different laboratories (Shaw et al., submitted). A pathology substudy was added to validate the participant’s diagnosis and round off the dataset on each person. Aficionados can download protocols and related information on these studies at ADNI’s add-on studies page.
For another, ADNI expanded to include amyloid imaging and genomics. Chet Mathis of the University of Pittsburgh School of Medicine heads the 11C PIB-PET substudy, with quality control going through the hands of Robert Koeppe at the University of Michigan, Ann Arbor. It has enrolled 106 participants who receive annual PIB scans either twice or three times, depending on their diagnosis and on when they joined. To date, baseline PIB scans on 101 of them (19 controls, 63 people with MCI, and 19 with AD) are uploaded on the LONI website; the remaining handful will go up this month. The participating sites are currently collecting year 1 follow-up scans; 37 of those are available at LONI already. About 47 percent of controls, 60 percent of MCI cases, and 90 percent of AD cases are PIB positive.
Here are PET images taken using Pittsburgh compound B that measure β amyloid accumulation. The are superimposed on MRI scans. The AD patient shows uptake of tracer throughout cortex, the control shows only non-specific white matter binding. Image credit: William Jagust
For this study, too, a complete comparison with functional PET imaging and MRI won’t be possible until all data are in. Here are the tentative insights from the data available so far: longitudinal data from ADNI, as well as from other centers such as the Karolinska group in Uppsala, Sweden, and the Austin Health Center in Melbourne, Australia, all agree that PIB retention in PIB-positive controls, MCI, and AD cases changes little from year to year. “Amyloid deposition is apparently a slow process that occurs over a decade or more,” commented Mathis. This confirms prior speculation based on postmortem studies.
ADNI data are beginning to show that FDG-PET is a more sensitive indicator of longitudinal change for AD than is amyloid PET. For mild MCI and especially the normal controls, the story is different. At those earliest stages, amyloid PET may be more sensitive than FDG-PET. That said, its link to cognitive decline remains to be firmly established, and on this issue amyloid imaging may benefit from combination with FDG-PET, Bill Jagust of UC Berkeley said at the International Conference on Alzheimer’s Disease (ICAD), held last July in Chicago.
How to interpret amyloid imaging data at these early stages is an area of active discussion. Different labs are working out how to decide whether a given person is “PIB positive” or “PIB negative” based on his or her scan. This is not trivial because amyloid deposition in the brain is a continuum. Wherever one draws the line, people just below the line have about the same amount of amyloid in their brains as people just above the line. The cutoff is artificial, but for practical purposes scientists sometimes have to place participants into those “positive” and “negative” boxes. Several approaches developed at Pittsburgh, Austin, UC Berkeley, and Washington University all roughly agree despite their quantitative differences, Mathis noted (see ARF related news story and Aizenstein et al., Amyloid deposition is frequent and often is not associated with significant cognitive impairment in the elderly, Archives of Neurology, in press).
Mathis emphasized, however, that the average PIB-positive controls look nothing like the average PIB-positive AD cases. PIB-positive controls have much less PIB retention than people with AD. “This is important to keep in mind,” he wrote to ARF. “One PIB-positive control in the ADNI data set looks very AD-like, but that subject is an exception. Focusing on that one control image is misleading of the PIB-positive control group as a whole.” The average PIB-positive MCI case, by contrast, looks similar to the average PIB-positive AD patient.
The other major add-on study focuses on the genomes of the 821 study participants. After ADNI got going in 2005, its principal investigator, Mike Weiner of UCSF, appointed geneticists from around the country to a working group led by Andrew Saykin at Indiana University in Indianapolis. Its charge was to ramp up ADNI’s originally modest design for ApoE testing and DNA preservation to a full genomewide analysis. This study aims to exploit the datasets of clinical, neuropsychology, imaging, and biomarker data in the same set of people in order to detect genetic variants that can explain some of the findings in those domains. For example, the search is on for genetic variants associated with the rate of progression of AD as measured by global and regional atrophy, or by metabolic changes, or genetic correlates of cognitive profiles and fluid markers. Besides informing early detection methods, this kind of data can also provide a foundation for future pharmacogenetic trials.
The working group selected a genotyping platform, planned data analyses, and secured funding through the Foundation of NIH. About a year ago, the genotyping study started up. It uses Illumina 610 Quad arrays, whose 620,901 markers, including SNPs, MCH markers, and copy number variants cover 90 percent of the human genome. According to Saykin, the genotyping itself is nearly done. “We anticipate that this will be entirely finished and quality control and basic analysis completed by the end of the year,” he wrote to ARF. A partial dataset—some three quarters of the samples with first-pass quality control—will go up on LONI this month. Eventually, the full data will become available on the NIH dbGaP website.
This is the first step. The second—analyzing this genetic data relative to the coming avalanche of neuroimaging and other phenotype data—is only just beginning. It will last beyond the arrival of the year 2 and 3 data, Saykin noted. And it’s complicated business. The data involved—multiple sets, each of them large—post tremendous computational and intellectual challenges. Imagine mapping more than 600,000 features and hundreds of thousands of voxels of MRI data per person, to pick just one example. To tame this data storm and draw meaning from it, the genetics working group has formed a set of multidisciplinary teams of imagers, neuroscientists, geneticists, computer scientists, and biostatisticians at several sites. It’s too early to ask for solid data. In the way of teasers, suffice it to say that Saykin’s group took a first crack at analyzing an available subset of data by examining genetic variants within Lars Bertram and colleagues’ Top AlzGene Results. According to Saykin, even just that first peek revealed some striking associations between known candidate genes, hippocampal volume, and gray matter density. But because the data are preliminary, he stayed mum for now on what those are.—Gabrielle Strobel.
This is Part 4 of a six-part series. See also Parts 1, 2, 3, 5, 6. Read the entire series [.pdf].
By common consensus of some 20 investigators contacted for this story from within and without ADNI, this behemoth study is working well overall. It is on plan, having enrolled all subjects. It is calling some participants for their year 3 follow-up visit, and its cylinders are cranking on data cleanup and analysis. Importantly, scientists generally applaud the standardization of procedures it has achieved across sites. But not everything went smoothly. “There have been some corrections and tune-ups along the way,” said Clifford Jack of the Mayo Clinic in Rochester, Minnesota, who heads ADNI’s MRI core and oversees quality control of the MRI images. “At a global level things are working well, but the closer you get to a large operation, the more chaotic it is.”
Snafus in the execution of a huge study offer learning opportunities for future studies. For example, one additional distributed consortium study modeled on ADNI, called DIAN, is gearing up and in its own planning has looked closely to ADNI. Beyond DIAN, ADNI has generated widespread interest in big-science studies. According to Andrew Saykin of Indiana University in Indianapolis, the ADNI model of data standardization and cooperation has come up even outside of Alzheimer disease in discussions of neuroimaging studies of psychiatric diseases, brain injury, and cancer. In this spirit, then, what could be done better next time?
“In retrospect, we should have allocated more funds to support the quality control process,” said Neil Buckholtz of the National Institute on Aging. “In terms of its basic structure and spirit of cooperation ADNI has done terrifically. But just tracking who is to get what procedure and that people come in at the right time, then making sure the data comes in at the time that it should, that it comes in the required form—those sorts of issues take more effort and person hours than we thought.”
A related issue is that the decision to make the imaging data publicly available almost instantly has subsequently raised questions about its quality. The concern is that if the data on LONI is raw, not processed, individual investigators who download it will have to clean it up themselves before analyzing it and introduce variation in this way. Some sites do their own reprocessing of ADNI data; for example, Nick Fox’s group in London uses differential bias correction (Lewis and Fox, 2004) on ADNI scans before measuring brain atrophy using their boundary shift integral method. That said, the ADNI imaging core teams do perform some preprocessing. The MRI imaging data come in two flavors, said Jack. The images become publicly available worldwide in their raw form as soon as a participating site uploads them. Also at that time, Jack’s team pulls those raw images to the Mayo Clinic, where scientists check their quality, correct errors, and follow up with the uploading site where they encounter a problem. “This is the data we encourage investigators to use,” Jack said.
What are those problems? Frequently they have to do with upgrades and subsequent software changes that have been performed at a local scanner unbeknownst to the ADNI scientists there, and become apparent through scan variations during ADNI quality control. Of the 84 scanners in ADNI, most are in clinical use at their respective hospitals, and ADNI scans take up less than a percent of their use, Jack said. Or sometimes the scans are acquired in the wrong way, and the participant has to return to the site for a re-scan. Another source of error can be the ADNI phantoms. These are a fleet of 66 identical water-filled objects that support calibration and preprocessing. They must be scanned along with a person’s MRI scan at every site. Other scientists noted privately that the phantoms had not performed quite as well as hoped for given their expense in terms of purchasing and scan time. Part of the problem is that they are not completely identical, and they can introduce a confound when one is dropped and has to be replaced. Some variation in the quality of the MRI scans arises from the different scanner models, and ADNI will address which model and field strength is the most suitable for ADNI’s goals. Given 20-20 hindsight, Fox and others noted that they might have spent more time in the preparatory phase to test scan sequences and test the value of the phantoms.
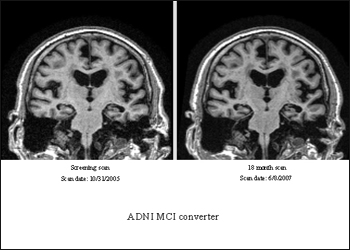
An ADNI participant who had an MCI diagnosis at study entry and again 18 months later (top images) showed relative lack of atrophy (view larger image) compared to a participant who initially was diagnosed with MCI but progressed to a diagnosis of AD 18 months later (view larger image). Image credit: Clifford Jack, Mayo Clinic, Rochester, Minnesota
ADNI’s biomarker study had its own share of “oops” moments while fine-tuning the operating procedures for this complex undertaking. Headed jointly by Les Shaw and John Trojanowski at the University of Pennsylvania Medical School in Philadelphia, the biomarker core personnel receive a dozen or so packages every day from the 58 participating sites, which send in urine and plasma samples (56 of those send in CSF, as well). “We expect by the end of the study to have received enough samples to create more than a quarter of a million aliquots of biofluid,” Shaw said. Every box has to be received, logged into the core database, thawed, aliquoted, and frozen into what’s casually called the “ADNI freezer farm” at UPenn. This, too, works well overall.
One of the bigger mishaps was that from the beginning of the study through March of 2007, some sites collected CSF samples into polystyrene tubes. Aβ sticks to this plastic, and use of those tubes has been shown to falsely lower CSF Aβ measurement by up to a third, according to Cindy Carlsson at the University of Wisconsin ADNI site. Carlsson, a geriatrician who conducts trials using CSF markers as outcome measures, discovered that the sterile CSF collection tubes in the ADNI lumbar puncture kits sent through a contract research organization were made of polystyrene. ADNI had provided each site with the polypropylene tubes needed for storing Aβ properly, but they were not sterile; hence, sites using a CSF drip technique that requires sterile tubes ended up using the wrong plastic. Carlsson added that ADNI fixed this problem as soon as it became apparent. When asked how many samples were affected, Shaw e-mailed to ARF: “We studied this very carefully, including by directly comparing CSF collected in polypropylene tubes to CSF collected in polystyrene tubes that are included in the standard lumbar puncture tray, and using an exposure time that most closely mimicked that for ADNI collections. We saw only minor decreases in Aβ42 and tau, none in P-tau, and hardly detectable [change] in the tau/Aβ42 ratio. This important issue was not a likely contributor to significant variability in our study.”
A second hiccup occurred around shipping logistics. It highlights the need for planning operating procedures down to minute details in such a large and complex study. The 58 local ADNI sites ship blood samples to the National Cell Repository for Alzheimer’s Disease (NCRAD), where the staff establishes cell lines for genetic studies on ADNI participants. According to NCRAD's principal coordinator Kelley Faber, ADNI samples often arrived at NCRAD on Saturdays, when NCRAD is closed. This might have been because participating sites ship some samples to NCRAD and others to the biomarker core at UPenn, which does receive shipments on Saturdays. On Saturdays, the ADNI boxes destined for NCRAD then got dropped off at a different lab at Indiana University. Not being part of the cell repository, that lab often refrigerated the samples, which is detrimental to the growth of the cell lines, Faber wrote to ARF. The NCRAD staff repeatedly instructed ADNI sites to hold samples drawn on Friday at room temperature and ship them on Monday, and also asked their local colleagues to store the Saturday arrivals correctly until Monday. The problem occurs less often now but, due to staff turnover in all those different labs, has not gone away. Were samples lost? “I don’t think many, if any, were lost, as we tried to give them extra TLC,” Faber wrote.
Moreover, samples sometimes arrive unaccompanied by their requisite form. This can be a major issue because the NCRAD staff then cannot easily double-check identifying information on the tubes. At other times, urine or CSF arrived at NCRAD instead of UPenn and had to be forwarded there. Overall, however, Faber noted that ADNI is going well. “Everyone was always friendly and willing to work together. The main issue was due to the number of sites and people working on the project. A lot has been learned from the ADNI study and will be used to improve future studies,” Faber concluded. Tatiana Foroud of NCRAD concurred that ADNI is going smoothly given its size and complexity. “We were very pleased to be a part of the ADNI project,” said Foroud.
Several scientists interviewed for this article regretted the timing of ADNI’s PIB-PET substudy. When the original ADNI grant was written in response to the request for applications the NIA had issued in October 2003, amyloid imaging was generating buzz at conferences and initial human data had been published (Engler et al., First human study with a benzothiazole amyloid-imaging agent in Alzheimer’s disease and control subjects. Neurobiol Aging. 2002;23 suppl 1:S429). But PIB was not formally ready for prime time, because the first widely noticed paper appeared in March 2004 (Klunk et al., 2004).
By the time ADNI’s amyloid imaging substudy was funded and set to go, ADNI had already enrolled so many participants that the substudy had to accept people who had undergone baseline FDG and MRI scans a year before, according to Chet Mathis of University of Pittsburgh School of Medicine. This cut into its ability to obtain three consecutive longitudinal scans on normal control and MCI volunteers, and to compare that side-by-side with ADNI’s other assessments. “We wish we had started sooner,” Mathis wrote to ARF. On the upside, the study made up the lost scans by enrolling more people than originally planned.
Finally, some scientists privately shared a concern that frequently accompanies big distributed science consortia beyond AD research. While they expect that ADNI will achieve its primary goals, they also say that it will necessarily do so at a low common denominator in terms of data quality. This concerns, for example, imaging resolution. That is because ADNI, despite everyone’s best efforts at standardization, must still absorb a considerable degree of remaining site variation. A related concern voiced privately is that ADNI may create the impression that the big problems are solved. In the process, it absorbs a large chunk of the available funding at the expense of more technically innovative, cutting-edge imaging and biomarker research in individual labs that might pay off later. That said, all sources agreed that the field has to have multisite data to move forward.
In most interviews, talk about fumbles and compromises came as part of a larger sense that overall, ADNI has worked surprisingly well. The problems underscore how daunting a task it has been to coordinate such a large undertaking, and how many obstacles had to be overcome. Here’s Sterling Johnson, co-principal investigator with Sanjay Asthana of the University of Wisconsin site. “There has been a high degree of planning, thoroughness, and standardization on every aspect of the complex data collection protocol.”—Gabrielle Strobel.
This is Part 5 of a six-part series. See also Parts 1, 2, 3, 4, 6. Read the entire series [.pdf].
Klunk WE, Engler H, Nordberg A, Wang Y, Blomqvist G, Holt DP, Bergström M, Savitcheva I, Huang GF, Estrada S, Ausén B, Debnath ML, Barletta J, Price JC, Sandell J, Lopresti BJ, Wall A, Koivisto P, Antoni G, Mathis CA, Långström B.
Imaging brain amyloid in Alzheimer's disease with Pittsburgh Compound-B.
Ann Neurol. 2004 Mar;55(3):306-19.
PubMed.
Around the time the North American ADNI started, similar efforts sprang up in countries across the globe. They are at various stages of planning or completion in Australia, Japan, several European countries, and most recently, China. The grand idea that there will be one openly accessible, interoperable global database on thousands of volunteers, all studied in the same standardized way, remains out of reach at this point as each national study works to resolve its own hurdles. But according to scientists heading these international studies, they share this goal, and it may be more a question of when than if it will come to pass. Here is a summary of ADNIs from around the globe.
This Sub-Volume Probabilistic Atlas (ASVPA) was obtained by merging the MRI volumes of a large family of AD subjects into a common reference space. White matter, gray matter, and CSF are modeled separately. The green and blue colors indicate the average distribution of the CSF and gray matter, respectively, across the AD population. For a detailed caption, search the LONI image database for ASVPA. Image credit: Laboratory of Neuro Imaging (LONI), UCLA
The Land Down Under: Don’t Call It ADNI!
Mention “Australian ADNI” to scientists from Down Under and they’ll bristle ever so slightly before explaining patiently that the Australian Imaging Biomarkers and Lifestyle Flagship Study of Ageing (AIBL) is anything but a clone of the American initiative. Funded at AUS$10 million by the Australian government, this three-year study started as an imaging and plasma proteomics effort with a dietary and lifestyle component. It only recently added a CSF measurement; whole genome screens and genetic analysis are being planned as well.
AIBL started without a mechanism in place to make its data fully and freely available to the research community at large, but this has since changed. According to Chris Rowe of the University of Melbourne, AIBL’s imaging data with matching neuropsychology and demographic data will be made available through the LONI website after a six-month moratorium. “Baseline data should be available in early 2009,” Rowe wrote to ARF.
AIBL started enrolling in 2007 and by now has completed baseline evaluation of 1,165 participants. They are grouped similarly as in ADNI, though with an additional group of people who complain about memory loss while appearing normal on neuropsychological test batteries. (American ADNI leaders are hoping to fill the gap between normal controls and MCI cases for ADNI2; subjective memory complaint is one attempt to capture that in-between group.) AIBL is at present beginning the 18-month follow-up of its patients, and at that point will request consent for a lumbar puncture. Longitudinal data on some 95 patients who were being studied before AIBL began are being analyzed already. AIBL conducts extensive amyloid imaging. It brings sophisticated software capabilities to image analysis and 3D rendering, for example, of how amyloid deposition spreads from cognitively normal to a full-blown AD load.
As to initial results, at the International Conference on Alzheimer’s Disease (ICAD) last July in Chicago, Kathryn Ellis of the University of Melbourne, with other AIBL colleagues, reported that the groups were well matched. AIBL scientists presented technical results on various ways of analyzing PIB-PET data. In addition, they reported that of 265 people who had undergone amyloid imaging in addition to MRI, 98 percent of AD cases and 60 percent of the MCI cases had an AD-like PIB pattern. Thirty percent of all healthy participants had brain amyloid, though that fraction was 50 percent among people carrying an ApoE4 allele.
One of 25 PIB-negative healthy controls and three of 10 PIB-positive healthy controls had converted to MCI. Five of 13 PIB-negative people with MCI had progressed to non-AD dementia (DLB or FTD), and 12 of 17 PIB-positive people with MCI had since advanced to AD. Kerryn Pike of Melbourne and her AIBL colleagues reported that healthy participants with brain amyloid performed worse on episodic memory tasks even though their overall neuropsychology scores were normal. To the Australian scientists, the data available up to this point would suggest that brain amyloid imaging can help pinpoint early memory impairment, or even latent AD.
In the Land of the Rising Sun, ADNI Is Coming Up
“I believe the ADNIs are the most important trend for bringing the fruits of basic research to the clinic,” Takeshi Iwatsubo of the University of Tokyo, wrote to this reporter. This is perhaps why the Japanese researchers have decided to clone ADNI (sort of). Iwatsubo, who leads a Japanese study that was modeled closely on the North American study, presented a summary with a slide presentation downloadable at adni-info.org.
Here are more recent updates, based on correspondence with Iwatsubo: the Japanese ADNI study engages 36 centers throughout the country. It is funded at about $3.5 million per year, to run for five years. Some 40 percent of that comes from a consortium of 10 pharma companies, whose representatives form an industry advisory board (ISAB) just as is the case for the North American ADNI. The Japanese ministry of economy, trade, and industry (METI/NEDO) and the Ministry of Health, Labor and Welfare (MHLW) together supply 60 percent.
The Japanese scientists intentionally designed their own ADNI to be as compatible with the U.S. ADNI as possible. This means the protocol employs the same method of MRI volumetry, uses the same phantoms, and the same schedule and type of clinical and neuropsychological batteries. Morihiro Sugishita, the leading neuropsychologist of J-ADNI’s clinical core, amended the existing Japanese versions of these tests to fit them to the English ones. According to Iwatsubo, this was no mean feat, but it’s nearly complete and raters have begun training for ADNI.
The Japanese scientists had the benefit of absorbing the gradual improvements of the N.A. ADNI into its original protocol. For one, the N.A. ADNI added amyloid imaging after it was already well underway, hampering this effort somewhat, whereas the J-ADNI implemented a standardized protocol for amyloid imaging from the get go. Some 13 sites out of the 36 will conduct amyloid imaging, because they have the capability to synthesize 11C-PIB or 11C-BF227 probes (BF227 is an amyloid tracer developed and increasingly widely used in Japan, see Furomoto et al., 2007). Some sites will invite patients from nearby centers, so that 17 sites in total and up to 30 percent of participants can obtain amyloid imaging, Iwatsubo wrote. For another, the N.A. ADNI expanded its initially limited CSF measurements after they turned out to be surprisingly promising. It also added a genetic add-on study later. The J-ADNI is planning on collecting CSF samples at multiple time points, aiming for some 40 percent participation, and Ryozo Kuwano at Niigata University is planning genome studies.
The J-ADNI is planning to analyze data jointly with data from the North American ADNI as soon as their own primary analysis is complete. To this end, the Japanese scientists will work with Laurel Beckett from the University of California, Davis, who heads ADNI’s statistics core. Unrestricted access to data as a public resource is another matter, however. The J-ADNI database will not be open to scientists worldwide, according to Iwatsubo. “However, it will eventually be possible to publicize all the data for wide use,” he added.
Planning for J-ADNI began in earnest in 2006, and the funding arrived in September 2007. Subsequent preparation and various training courses then preceded enrollment, which began last month. The J-ADNI will study 150 normal controls, 300 people with MCI, and 150 with early AD by 2010. It’s starting well, Iwatsubo wrote. “Japanese clinicians/researchers, lay people, government, and pharma, especially global pharmas that are starting trials in Japan, are very interested in J-ADNI. Some sites are flooded by normal volunteers who wish to be enrolled.”
The Old Country: Pilot a Success, But Europe-Wide ADNI Won’t Fly
In Europe, the story of ADNI is less straightforward. Academic centers in seven countries have jointly tested the ADNI platform in a pilot study funded by the U.S. Alzheimer’s Association. They found the platform to be feasible for Europe to adopt, but the follow-up support for a full-fledged European ADNI fell short. Instead there will be national initiatives.
At the International Conference on Alzheimer’s Disease (ICAD) last July in Chicago, Giovanni Frisoni from Fatebenefratelli in Brescia, Italy, presented details from the European pilot ADNI, which also appeared in print the same month (Frisoni et al., 2008). In short, academic centers in Amsterdam, Brescia, Copenhagen, Munich, Rome, Stockholm, and Toulouse had banded together to try out whether the N.A. ADNI platform of collecting clinical, neuropsychological, structural, and functional imaging together with biochemical information in a pooled way would work for them.
Each center recruited three patients each in the control, MCI, and AD groups for one baseline assessment. No follow-up was planned. For the clinical assessments, the European study translated the forms of the U.S. ADNI into six different languages. On imaging, the volunteers submitted to a 1.5 Tesla volumetric scan and a diffusion tensor scan. Unlike the N.A. ADNI, the European ADNI also took a resting fMRI measurement, but no amyloid scan. For calibration, they used three human “phantoms” who traveled from center to center to be scanned in each of the participating machines. Three quarters of the participants agreed to a lumbar puncture.
These are the results: the European patients matched the North American ones well in their clinical measures and cognitive performance. A few differences showed up (e.g., the Europeans were a tad more depressed), but they were small. On the imaging results a manuscript is in preparation, and on the biomarker results a paper is submitted (Buerger et al.). In a nutshell, the results were comparable to the American ADNI. Hippocampal atrophy increased from normal to MCI to AD; white matter abnormalities did not. CSF total tau increased and Aβ42 decreased as expected from normal to MCI to AD. “We came out with study groups that from a clinical, functional, and neuropsychological standpoint are remarkably similar to those of the American ADNI,” Frisoni later wrote to this reporter.
The results of this pilot study support the validity of the American ADNI platform, and a larger European study could be set up fairly quickly based on this model, Frisoni said at ICAD. But it most likely will not. Due to political and structural reasons, a large European ADNI with pooled, openly accessible data is unlikely. Instead, there will be national efforts. “National efforts are more of a necessity than a choice, arising from the much more fragmented way research is funded at the European Union level,” Frisoni wrote.
In Germany, Italy, and France, scientists are setting up their respective networks that Frisoni hopes will choose the ADNI platform to collect multicenter prospective data. In addition, some ADNI-related initiatives already exist in Europe. For example, an EU-funded multinational, public-private initiative already uses an ADNI-compatible MRI protocol. Called AddNeuroMed, it is coordinated by Simon Lovestone at King’s College, London (Lovestone et al., 2007). At ICAD, Christian Spenger of Stockholm’s Karolinska Institute reported that the AddNeuroMed network had enrolled 383 subjects in two years of operation thus far, and he emphasized the study’s focus on quality control. Furthermore, academic centers in Brescia, Amsterdam, and Stockholm are presently building an electronic infrastructure that aims to support advanced computational analysis of ADNI-compatible images. Called neuGRID, it receives European Union funding of €2.8 million.
Whether these separate efforts will consolidate to become compatible with the American and Japanese ADNI, or whether they will remain different is an important but unresolved issue, Frisoni noted. Ditto for the question of whether their data will be openly available. “Appropriate coordination of all these efforts would enhance the impact of EU research,” Frisoni wrote, adding that the political hurdles on the way are considerable.
New Kid on the Block: ADNI-like Studies in China
Chinese researchers have not stood idly by while interest in comprehensive natural history studies of AD has grown elsewhere. In fact, they have started several similar studies. These initiatives come against a backdrop of estimates that the percentage of people older than 60 in China’s population will triple by the year 2050, from about 10 percent now to 30 percent then. Of two multicenter initiatives described here, one is a biomarker study similar to the North American ADNI in design; the other has a more epidemiological bent and focuses on MCI, but its overall idea is the same as ADNI’s.
The principal investigator of one study is Jun Xu, who was a postdoctoral fellow at the University of Pittsburgh before joining the faculty at the Nanjing Brain Hospital and Nanjing Medical University, China, where he is vice dean of the Department of Neurology. His study is a government-funded effort in Eastern China that at present includes 10 centers located in Nanjing, Shanghai, Beijing, Guangzhou, Chengdu, Xi'an, Hangzhou, Wuhan, and Fuzhou. Co-principal investigators are Wu-hua Xu (no relation) at Jinan University 4th Hospital in Guangzhou, and Yong-an Sun at Peking University 1st Hospital in Beijing. According to Xu, this study started up in May 2008 and has to date enrolled 100 of a targeted 500 patients. Of those, 200 will be normal controls, 200 have amnestic MCI, and 100 probable AD. According to Xu, this study uses much the same protocol as the American ADNI, with the express intention of gathering data using the ADNI platform of standardized assessments. The study includes clinical and neuropsychological assessments, MRI, FDG-PET, CSF, and plasma biochemistry. Due in large part to its expense, amyloid imaging is not part of the current protocol, nor are whole genome screens at this point in time, Xu wrote to ARF.
In one marked difference to the other ADNIs, this Chinese study is planned to run for 20 years. That means the study places a particular emphasis on observing the long-term natural history of disease in its participants, and hopes to learn a great deal from the 200 volunteers who were cognitively normal at study entry.
Xu wrote to ARF that the Chinese investigators aim to make their data publicly accessible, much like the North American ADNI data are on LONI, but he added that the requisite software remains under security consideration and still awaits approval. Likewise, Xu noted that the Chinese investigators are interested in connecting their data with the American data pools to enable joint analyses and boost power. On this goal, as well, structural, legal, and privacy issues still need to be sorted out.
How did Xu develop his interest in ADNI? The Internet made it easy. After his return to China, Xu simply kept up to date through the websites of ADRCs, the NIA and ADNI-info.org, LONI, and took it from there. The Chinese investigators are holding a symposium to discuss enrollment and screening data this December. According to Wu-hua Xu, this study is looking to engage more specialists in China and open to interacting with North American ADNI colleagues.
A separate, five-year study that focuses on mild cognitive impairment is gearing up under the direction of Jianping Jia. Jia directs the Department of Neurology of Xuan Wu Hospital of Capital Medical University in Beijing. This study is part of China’s effort at early detection of dementia and MCI. Called the Chinese Dementia and Mild Cognitive Impairment Longitudinal Study, it received funding in 2007 from the Ministry of Science and Technology and the Ministry of Health of the People’s Republic of China. Covering 12 provinces in five geographic regions of the country, this is a community-based epidemiology and natural history study of MCI in China. Its goals are to determine fundamental datasets on prevalence and subtypes of dementia in China, to find risk and protective factors, and to identify predictors for MCI conversion. It also aims to establish normative data for cognitive measures and find cognitive tests that are sensitive for MCI, according to Maria Carrillo of the Alzheimer’s Association, who is working to coordinate worldwide ADNI efforts. To this end, the study will gather data on risk factors, medication, and cognitive impairment history. Using annual follow-up visits, it will include a range of assessments, such as neurological, neuropsychological, as well as some biological data in blood and neuroimaging. Genetic tests for ApoE and FAD genes are also planned.
The study this year began screening a sample of 30,000 elderly people in communities and hospitals, but how many will be enrolled has not been calculated yet, Jia wrote to ARF. “We are hoping they will join the WW-ADNI effort. We are in the planning process of having a WW-ADNI meeting in Japan in November 2009, and these Chinese investigators will of course be invited,” Carrillo wrote.—Gabrielle Strobel.
This article concludes a six-part series. See also Parts 1, 2, 3, 4, 5. Read the entire series [.pdf].

{kind=link}
{kind=link}
Comments
No Available Comments
Make a Comment
To make a comment you must login or register.