The general media in the U.S. and abroad have discovered the story of autosomal-dominant, early-onset Alzheimer’s disease, showcasing its human face while raising awareness among large international audiences. Meanwhile, researchers in the South American nation of Colombia and the U.S. are racing to prepare for therapeutic trials in dozens of such families afflicted with this particularly dreadful form of AD. They argue that therapeutic success in rare mutation carriers destined to develop AD will serve as a stepping stone toward preclinical trials of sporadic AD, which afflicts millions.
Along the way, they are publishing new research about the asymptomatic phase of AD. Reporting from a recent expert meeting of scientists and regulatory experts held in Washington, D.C., Gabrielle Strobel pulls together current developments on this frontline of the fight against AD. While research is gearing up, a new charitable foundation invites donations and volunteer work to support Colombian families, who frequently care for several loved ones at a time.
Colombians Come to Fore in Alzheimer’s Research, Mass Media
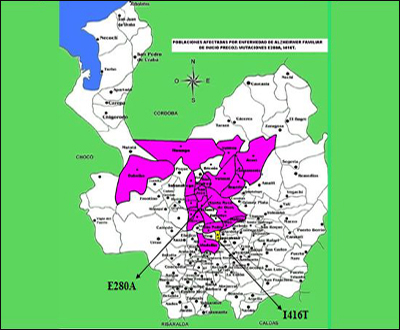
If you follow Alzheimer’s disease research at all, chances are you have heard of the families in the South American nation of Colombia who comprise the largest known population stricken with early onset autosomal-dominant Alzheimer’s disease (ADAD). Passing relentlessly through the generations in a lineage of some 5,000 people, a single-nucleotide flaw in the presenilin-1 gene called the Paisa mutation is stalking some 25 extended families in the hilly Antioquia region of the northwest of the country. But you may not have fully caught on to how these families—after 30 years of giving time and tissue to research—have finally captured the sustained interest of researchers and drug companies around the world in a serious and broad-based way. That interest results from a combination of partnerships, new research, and media attention. It has created a new sense of hope among the families, which scientists and the pharmaceutical industry are now challenged to fulfill.
Town of Yarumal, Colombia. Image credit: Felipe Barral/CNN
Yarumal, Colombia. Image credit: Felipe Barral/CNN
Medellin, Colombia. Image credit: Felipe Barral/CNN
The families’ recognition among drug developers is growing in part because widespread frustration with clinical trial failures converges with the realization that this population might just help the whole field turn things around. But that is not the only reason. Francisco Lopera at Universidad de Antioquia, Medellin, has for most of his career been the families’ physician-researcher, the chronicler of their disease, and their beacon of hope. In 2009, Lopera teamed up with U.S.-based scientists in a collaborative drive toward prevention trials that is gaining momentum within the U.S. and European academic, drug development, and even regulatory AD community.
In Medellin itself, Lopera has built a group, called Grupo De Neurociencias De Antioquia, of some 50 neurologists, neuropsychologists, nurses, basic neuroscientists, junior researchers, and students. In the past year alone, they have prepared for anticipated prevention trials by screening 800 people for participation. That is an unprecedented number for any kind of human research in ADAD. Moreover, the researchers published four papers in the past six months, most recently on February 3 in Lancet Neurology (Acosta-Baena et al., 2011). Three of these papers are characterizing the preclinical phase of familial AD at earlier stages and in greater depth than was previously possible, by way of both paper-and-pencil tests and biomarker studies. The goal of this research is nothing less than a comprehensive description of memory, brain imaging, and fluid biomarker changes going back to the point in life when a mutation carrier first diverges on each of these measures from their non-carrying siblings. If necessary, and as appropriate, the researchers will trace those markers back to childhood, Lopera said. (For a summary of these new data, see Part 3 of this series.)
The last, and in some ways perhaps most powerful, ingredient to the family’s changing situation has been a flurry of media attention as their plight and their dignity have captured the imagination of both print and television journalists in Colombia, the U.S., and around the globe. In June of 2010, a New York Times story by Pam Belluck, a reporter who accompanied the Alzheimer’s Prevention Initiative (API) researchers on a visit to Antioquia, ran a haunting online video for streaming in four parts. Scientific American covered the API as well. On 29 January 2011, a feature-length documentary film by Felipe Barral, an artist and producer for CNN International, started airing on that channel and on CNN en Español (see ARF news flash and CNN website), with repeat shows all through February (see ARF related news brief). To the community’s disappointment, CNN domestic never aired the documentary, but it did upload it for screening in four parts on CNN.com (play Part 1, Part 2, Part 3, Part 4). On 17 February 2011, Sanjay Gupta talked about the API on Katie Couric’s “CBS Evening News.” Missed it? Catch the segment here. Last December, Colombia’s national newsmagazine Semana profiled Lopera in a year-end issue on important national leaders (see online version). Other Colombian newspapers ran stories as well (see El Espectador.com).
Colombian family with CNN cameraman. Image credit: Felipe Barral/CNN
Felipe Barral
CNN cameraman Greg Kilday films Kate Preskenis. Image credit: Felipe Barral/CNN
On the science front, things are moving as well. On 7 January 2011, some 80 scientists from the U.S. and European medicines regulatory agencies, the biopharma industry, academia, nonprofit foundations, and the government met in Washington D.C. for the latest round of planning called by the Alzheimer’s Prevention Initiative (Reiman et al., 2010). This was the third such gathering, each larger than the previous one. The API is widening the circle of participants in an inclusive and intensely collaborative joint effort to start what Eric Reiman calls an “era of prevention research.” Reiman, Pierre Tariot, and Jessica Langbaum of the Banner Alzheimer’s Institute in Phoenix, Arizona, lead the API with Lopera and colleagues in Phoenix and Medellin. The first API meeting, in October 2009, gathered mostly academic advisors. The second meeting, in January 2010, branched out to include industry representatives. Both groups roundly endorsed the initiative. For a detailed introduction to the API, see ARF related series.
At this most recent meeting in D.C., the group met for an update on how far the API has come in the past year (see Part 2 and Part 3), and for in-depth discussion with regulators of how best to design trials in this unique population (see Part 4 and Part 5). The day left the ball in the court of the pharma industry. Its representatives got answers to some of the questions they had asked in January 2010, and they heard a resounding plea to find ways of working collaboratively towards shared, creative trials of their most promising compounds (see Part 6).—Gabrielle Strobel.
A Neurologist’s Devotion Puts Familial AD Research Onto New Plane
What has the Alzheimer’s Prevention Initiative accomplished this past year? In February 2010, Eric Reiman and Pierre Tariot of the Banner Alzheimer’s Institute, Phoenix, Arizona, along with Kenneth Kosik of the University of California, Santa Barbara, traveled to Medellin, Colombia, to work onsite with Francisco Lopera at Universidad de Antioquia in Medellin. Lopera had begun working with families carrying the presenilin-1 Paisa mutation as early as 1980, first with a group in Belmira, and then spreading to include 25 extended families that encompass 5,000 members. The majority live in Medellin, Angostura, Yarumal, and Santa Rosa de Osos; others live in towns and villages in surrounding areas, including Belmira.
Francisco Lopera, above left, began working with this family in Belmira in 1980. Image credit: Francisco Lopera
Image credit: Francisco Lopera
During this visit, the API collaborators worked on setting up infrastructure for future trials and the accompanying biomarker research, as well as on procedures for screening and enrolling participants. They met families in different villages surrounding Medellin. “We consider the families partners in this. They moved us deeply. You cannot leave Colombia without being fully committed to their cause,” Reiman told the attendees of an API workshop held 7 January 2011 in Washington, D.C. Scientifically, researchers working with familial AD in API and in its sister initiative, the Dominantly Inherited Alzheimer’s Network (DIAN), argue that their work will generalize to the millions of people with sporadic late-onset AD. But what sets them apart most is that they confide being gripped on a deeper, personal level with a sense of obligation to relieve the families’ suffering. “Working with autosomal-dominant AD changes you as a person,” said Bill Klunk of the University of Pittsburgh Medical Center. Klunk is part of the DIAN, and for many years has developed amyloid PET imaging in such families as a step toward preclinical drug trials in them and, eventually, in all AD.
Since last February, Lopera’s team at the University of Antioquia has screened around 800 family members for trial participation. The scientists enrolled them with neuropsychology tests, clinical exams, blood draws, as well as CSF sampling for fluid marker measurements and volumetric and functional MRI scans in a growing subset. The University of Antioquia has MR scanners; a cyclotron for amyloid imaging radioligand synthesis will be up and running soon, said Reiman. The goal is to screen another 750 relatives in 2011, aiming for 2,000 enrolled in total. About 660 of them are expected to carry the Paisa mutation.
These are huge numbers by the standards of autosomal-dominant AD research. Most prior published studies in families around the world had far fewer than 20 carriers. Even the DIAN, which to date has enrolled 150 participants to its ongoing observational studies and planned treatment trials in the U.S., Australia, and the U.K., is hard-pressed to match that number because most autosomal-dominant Alzheimer’s disease (ADAD) families known to science are small and far flung.
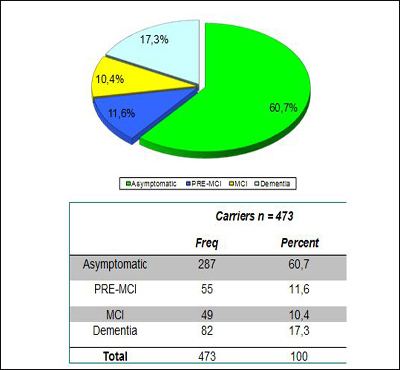
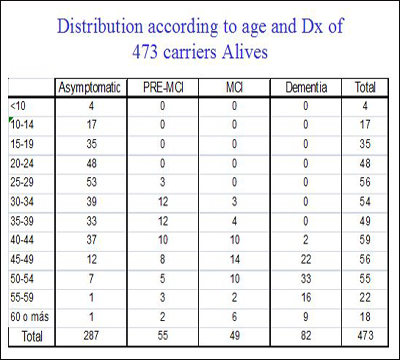
At the D.C. meeting, Lopera told the regulators, researchers, and funders that of the total Paisa lineage of 5,000, his team to date has studied 2,440 descendents. Of those, 1,107 escaped the mutation, 577 carry it, and 756 were not genotyped. Of the last, 506 are alive, as are 473 carriers and 1,096 non-carriers. For a precise breakdown of what stages of AD these carriers are in, and how old they are, Lopera generously made slides available for Alzforum readers. His data show that a small majority of the carriers enrolled so far are asymptomatic at present and are younger than 35. This is the age at which the researchers can now detect the very first signs of a subtle memory deficit (see Part 3 of this series). The cohort to date has about 100 carriers each in their twenties and thirties.
Image credit: Francisco Lopera
Image credit: Francisco Lopera
Lopera further said that of the 800 people screened so far, nine in 10 intend to participate in clinical trials. This is important, because in the U.S. and Europe, researchers historically have cited difficulties in finding willing trial participants among autosomal-dominant Alzheimer’s disease (ADAD) families. This was true especially in the past, when coordinated efforts to approach trials in a partnership with families did not exist. DIAN is changing this reluctance in its participating countries, too. At the D.C. conference, DIAN investigators Nick Fox of University College, London, and Randy Bateman of Washington University, St. Louis, reinforced Lopera’s point, saying their study participants, too, want to enter treatment studies. Lopera emphasized that relatives say they want such trials even though they understand that the trial may come too late for themselves. Possibly helping their children is motivation enough for them (see also ARF related London story).
Pierre Tariot, Kenneth Kosik, F. Manes, and Francisco Lopera met with families in Angostura, Antioquia, in February 2010. Image credit: Francisco Lopera
Yakeel Quiroz is a graduate student at Boston University who did undergraduate work with Lopera. She still collaborates extensively with Lopera, and meets, comforts, and studies relatives of the Paisa mutation families. At the D.C. conference, Quiroz said, “When you work with these families, you see their emotional and financial burden. It is worse in familial than sporadic AD, because frequently more than one relative is sick at the same time. We see families that have three or four patients at different stages.” Indeed, a CNN documentary about these families showcased a woman, who is a nurse, and cares for a brother and a sister who are both mute, immobile, and require 24/7 care. The sister has been in this condition for nine years. Julie Noonan, an unaffected sibling of a U.S. family with FAD that was featured in the CNN documentary, also became a nurse after growing up with a mother who had succumbed similarly slowly to the disease. In the Colombian families, the disease starts in a person’s thirties, when people are providers to young children.
Edilma in Yarumal, Colombia. Image credit: Felipe Barral/CNN
Julie Noonan Lawson and Kate Preskenis. Image credit: Felipe Barral/CNN
What do the families want in return for the risk they take on with these trials? For one, they ask that the drugs have a reasonable safety record, Lopera said. This issue generated discussion at the D.C. conference, as API leaders asked regulators just how safe a drug must be for secondary prevention trials in FAD families. Generally, in the AD field, conversations about this topic are dominated by intense apprehension that an adverse drug effect in an outwardly still-healthy carrier could derail a company’s whole development program of a drug in question (see eFAD essays). That worry has held back such trials in the past.
To be mindful of both the families’ safety and skittish drug companies, the API leaders began their planning on the assumption that a drug for an FAD prevention trial would have to be chosen primarily on the basis of a strong safety record, even though in practice, that might come at the expense of the drug’s scientific rationale and mechanistic promise. Not necessary, the regulators from both the U.S. Food and Drug Administration and the European Medicines Agency said. Russell Katz from the FDA called the concern being expressed about safety “somewhat overblown. The people in this PS1 population have a very bad disease. You need no more safety data than for any relatively large long-term study. Usually for that, you have early Phase 2-type data of some duration. That would be good enough even though these patients are apparently cognitively normal before they take the drug.” Cristina Sampaio of the EMA said, “I very much agree.” Usually in drug development, short-term safety tests in healthy volunteers precede longer trials in patients, but in this case it is logical to flip the order around such that short-term safety data gained in sporadic AD patients could precede longer-term trials in still-healthy mutation carriers. “This is a matter of common sense more than regulation,” Sampaio said, expressing confidence that a practical solution could be found. (For more of the regulators’ stance on preclinical AD trials, see Part 4 and Part 5.)
For another, the families asked that any successful drug be made available to their families after the trial ends. They also want researchers to offer a trial for their already symptomatic relatives, lest they be forgotten in the enthusiasm for preclinical trials. The families request information about the risk potential benefits, and mechanism of action of the candidate drugs. But by and large, they support the project enthusiastically. “The families are sick and tired of AD; they want to end it,” Quiroz said. They even express a sense of national pride that their country could contribute an important piece toward solving the world problem of AD.
While the families asked for nothing material, anyone working with them can plainly see that their needs are tremendous, said Tariot. They need adult diapers, walkers, anti-dementia medications, antidepressants, and antipsychotics, for example. Medical aids can relieve the patients’ symptoms and ease the daily work of caring for an incapacitated spouse or sibling year in and year out while the loved one’s middle-age heart remains strong. To help raise funds for caregiving supplies, Quiroz has set up a private foundation. Called the Forget Me Not Initiative, it offers ways of donating funds or connecting with Quiroz and colleagues to organize a fundraiser.
Incidentally, Quiroz pointed out, while the families are less educated and poorer than people in the U.S. or Europe, they are industrious and highly functional. They give devoted care to their relatives. Indeed, in their book The Alzheimer’s Solution, Prometheus Books, 2010, coauthors Kenneth Kosik and Ellen Clegg describe the quality of caregiving in this Colombian population as a starting point to argue for a more integrated approach to dementia care and prevention in the U.S. (see also ARF related CFIT story and Webinar). For the purposes of API, Quiroz said that the families are fully capable of complying with protocol requirements.
The API collaboration with the Banner Institute has given the families renewed hope, Lopera told ARF. Of the relatives who came to him for care and research decades ago, some had dropped out over the years because he could offer them no prospect of real change. But after the collaboration with the Banner Institute began last spring, word went around, and now old faces are returning and relatives and new families are coming forward. “Of the 800 people we screened last year, 450 are new,” Lopera told ARF.
This renewed engagement raises the stakes for everyone. Hopeful once again, the families are paying close attention to the project. “They now see they are not alone. They know there are many scientists in the world who are thinking of them,” Quiroz said. This makes getting started with therapeutic prevention trials a shared responsibility, the API researchers said. They called upon companies to participate not just by attending the API meetings, but also by making treatments available and collaborating actively. At the API meeting in Washington, Quiroz translated a message a patient in his early forties had given her. “I know for me it is too late, but please help my children.” This man is starting down the path of MCI, and he knows what will come for him, Quiroz said. (See Part 3 for new research data.)—Gabrielle Strobel.
Detecting Familial AD Ever Earlier: Subtle Memory Signs 15 Years Before
Recent findings have strengthened the scientific underpinning of the Alzheimer’s Prevention Initiative (API). On 3 February 2011, Natalia Acosta-Baena and colleagues reported in the Lancet Neurology that they were able to capture a clear decline in cognition starting in people’s early thirties in the largest-known population with autosomal-dominant Alzheimer’s disease. They define an earlier disease stage prior to what is called pre-MCI, in effect pushing the line of detectability back toward younger ages by some four years. Two other papers go in the same direction. Last July in the journal Brain, Mario Parra and colleagues published a new test that appears to detect a specific visual memory deficit perhaps even earlier, at ages when mutation carriers perform as well as controls on standard neuropsychometric tests. And in last December’s Annals of Neurology, Yakeel Quiroz and colleagues report the first of what is expected to be a wave of preclinical brain imaging findings. Carriers in their thirties, while still performing the memory test at hand as well as non-carriers, drive their hippocampus harder to achieve that parity. Together, these three papers push back the preclinical phase of AD that is amenable to detection by way of neuropsychology and imaging. They characterize the 20 to 15 years prior to dementia in greater detail. All three are coauthored by Francisco Lopera, a neurologist at Universidad de Antioquia, Medellin, Colombia, who has characterized and cared for the largest known population in the world with autosomal-dominant AD (ADAD) inherited via a presenilin-1 mutation.
Being based in South America, Lopera is little known among researchers elsewhere, but in fact, his group has published quality research in highly regarded journals for decades. For example, just last December Lopera published results of a collaboration with Markus Glatzel at University Medical Center in Hamburg, Germany, and researchers at Novartis in Basel, Switzerland, and the University of Barcelona, Spain, which found that the cerebellum is more affected in AD than previously thought, raising questions about its widespread use as a reference region; see Sepulveda-Falla et al., 2010.
The Acosta-Baena, Parra, and Quiroz papers reflect different facets of the field’s combined push toward refining the still-sketchy description of the pre-dementia phase of AD (Acosta-Baena et al., 2011; Parra et al., 2010; Quiroz et al., 2010). This is necessary to upgrade clinicians’ toolkits for measuring whether an experimental drug does any good in future pre-symptomatic trials. Toward that goal, Jessica Langbaum of the Banner Alzheimer’s Institute in Phoenix, Arizona, reported a fourth sign of progress at a 7 January 2011 conference of the Alzheimer’s Prevention Initiative held in Washington, D.C. Together with colleagues at Banner and biostatistician Suzanne Hendrix of Pentara Corporation in Salt Lake City, Utah, Langbaum and the team built upon Hendrix’s previous findings that the trusty but imperfect ADAS-Cog package of neuropsychometric tests performs better in clinical trials of MCI and AD if the scientists remove certain components that add variability and dilute the battery’s predictive power (Hendrix and Wells, ICAD 2010). With these and other efforts, scientists should soon be able to put together a serviceable package of outcome measures for secondary prevention trials, Lopera said. Read on for a summary of the three papers and Langbaum’s study.
Fifteen Years of Observation on 449 Carriers
Many scientific groups these days are trying to define the symptoms and biomarker changes in the years before dementia. “The diagnosis of AD is marching leftward on the time scale,” said Paul Aisen of the University of California, San Diego. Different groups take different approaches, and, consequently, parallel terminologies coexist in the field to denote otherwise similar stages of pre-dementia (Dubois et al., 2010; ARF related ICAD story). In the Lancet Neurology paper, Lopera and his team framed their study in the language of mild cognitive impairment (MCI). Because it is clear that some cognitive deficits precede MCI as defined by its diagnostic criteria, the stage of pre-MCI has been suggested (Reisberg et al., 2008). In the general population, the MCI category is heterogeneous because a significant fraction of patients do not progress to AD or even revert from MCI back to normal. In contrast, all previous longitudinal studies of familial AD have noted a continuous, gradual decline, making inherited AD an ideal model to characterize the long slide into dementia from its very beginning.
Each of the previous familial AD studies was small. In this paper, the Colombian scientists retrospectively analyzed descendents of the largest-known cohort of autosomal-dominant AD, including 1,784 patients age 17 to 70 who came to Lopera for treatment and research between 1995 and 2010. This study is by far the biggest study of its kind. Four hundred forty-nine people carried the E280A Paisa mutation. Four hundred ninety-nine non-carriers served to establish normal parameters on the expanded CERAD battery of cognitive tests that the scientists administered to the participants at follow-ups every other year where possible. The scientists modified and added some tests to the U.S.-based CERAD battery to adapt it to the language and educational differences of this Colombian population. These people have from one to 11 years of education and low income, though as a group they function well in life.
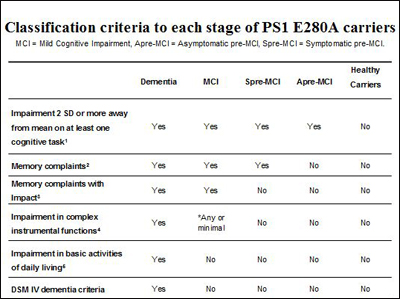
What were the very first signs the researchers saw? Memory loss in the early thirties, Lopera said. To describe this finding, the scientists ended up splitting the published pre-MCI category into two distinct stages. “We were originally looking only for MCI and pre-MCI, but when we analyzed the data, we found that there are people who are otherwise asymptomatic but in one test fall short by two standard deviations. They do not yet meet criteria for pre-MCI,” Lopera told this reporter. These are people who do not complain of memory problems yet and have no functional impairment, but they do fail one objective measure in the CERAD-plus battery. Seventeen people fell into this group in this analysis. Anecdotally, Dominantly Inherited Alzheimer Network (DIAN) investigators have noted that in their hands, too, some otherwise asymptomatic participants send up an early flag by doing poorly on a single test. Longitudinal research on both the DIAN and Paisa cohort is ongoing.
How did the Paisa mutation carriers progress from that first cognitive deficit? Some four years later, around age 38, they tended to meet published criteria for pre-MCI; six years later, at age 44, they had progressed to MCI; and five years later still, around 49, to dementia. They then live with dementia for an average of 10 years. The very first deficits can show up in a variety of memory domains.
Overall, the cognitive profile of this population is very similar to that of sporadic AD, Lopera said. This means that about 25 years pass between this first (at present) measureable sign of a cognitive problem and death from AD. The age at each stage varies somewhat from person to person, but the range is relatively small, around three to four years.
Presented at a 7 January 2011 API conference in Washington, D.C., this slide recapitulates the stages of autosomal-dominant AD in the Colombian carriers of the presenilin Paisa mutation, formally published on 3 February 2011. Image credit: Francisco Lopera
“The systematic description of the natural disease history in this cohort provides a framework for the design of studies of preventive intervention,” writes John Ringman of the University of California, Los Angeles, in a comment in the same issue of Lancet Neurology. Ringman leads a DIAN site and has studied different presenilin-1 families in Southern California and Mexico with cognition and biomarker measurements (e.g., Murrell et al., 2006).
A New Test
The Acosta-Baena study pushes back the time of the first detectable sign of AD compared to a previous, smaller analysis of people with the Paisa mutation, which had pegged subjective memory complaint to around age 38 (Ardila et al., 2000). But it is not the last word on the matter. The protocol used in this study was designed for dementia; it is less sensitive in the preclinical years than newer tools scientists across the field are developing. One such tool comes from Lopera’s group itself. Probing a fundamental function of visual short-term memory that is not part of any standard psychometric battery, the new test shows a robust effect already during a carrier’s early thirties, the age at which they also show the first decrement in a conventional memory test that Acosta-Baena et al. report.
Developed by Mario Parra, then a student in Lopera’s group, this new tool tests a person’s visual short-term memory binding. That is a memory function that allows people to “bind” together moment-to-moment changes in shapes and colors in their memory temporarily, for example, to remember whether they just took the yellow or the white pill. It is different from remembering stable properties of the world, for example, the shape and color of your mailbox or of the school bus. Previous research had shown that short-term visual memory binding is independent of aging. This seemed an advantage over other associative learning tests that are widely used in AD research, because these do decline with normal aging and hence make it more difficult to pin a change firmly on preclinical AD.
To test whether visual short-term memory binding flags future AD early, Parra enrolled 22 symptomatic Paisa mutation carriers, 30 asymptomatic carriers in their thirties, and 30 matched non-carriers. He subjected them both to a fleet of nine established memory tests and to a binding test in which they learned and then recalled both the shape and the color of polygons on a computer screen. Asymptomatic carriers were not statistically different from the non-carriers on any of the standard neuropsychological tests (though they trended downward a little), but they did have striking trouble with the binding tests. They were able to recall shapes all right; they were able to recall colors all right, but they could not bind the two together in their memory. The non-carriers could. In the binding task, the asymptomatic carriers performed just like symptomatic carriers. Among these 10 tests, then, only short-term visual binding distinguished the young asymptomatic carriers from non-carriers, and it did so clearly, the scientists report.
The test is surprisingly sensitive and specific for AD, Lopera said. Unlike other neuropsychometric tests, it does not vary with socioeconomic background or education. In its published form, the test is not practical because it takes some 80 minutes to administer. But since then, Parra has developed a 15-minute version, which in unpublished tests of 40 carriers and 80 non-carriers works as well, Lopera said. Like any new finding, this will have to be reproduced independently in other cohorts before scientists across the field accept it. Lopera hopes that will happen. Previous research indicates that visual short-term binding may well detect sporadic Alzheimer’s at the pre-MCI stage, too. Ongoing testing in the Colombian families will show whether this test distinguishes carriers from non-carriers even earlier than the two standard deviation decline reported as the first sign by Acosta-Baena et al.
There is a desire across the field to agree on tests that are sensitive and robust in the earliest stages of the AD process. Regulators keep saying, and scientists recognize, that cognitive tests will be needed to bridge the gap between expected drug effects on preclinical biomarkers and the eventual clinical benefit that matters to the patient and that allows a new treatment to be approved. It is not realistic to show that a drug hits a target in the desired way in a wholly asymptomatic person, and then wait many years to see if the clinical diagnosis changes. Change in early cognitive tests should accompany biomarker outcomes, or follow on within a practical time period. Between these recent papers and other research, Lopera sees a combined episodic memory and executive phenotype that should yield suitable tests soon. (Visual short-term binding is an episodic memory function.)
Imaging Markers in Paisa Mutation Pedigrees
What about biomarkers in these thirty-something carriers, anyway? The API researchers are gearing up for an ongoing study in which they intend to characterize the major markers in the Colombian population across all age ranges, first cross-sectionally and then longitudinally going forward. They aim to pinpoint for each marker at what age carriers first diverge from non-carriers, and to track the changes from there to dementia. To date, one brain imaging paper in the December 2010 Annals of Neurology and a Society for Neuroscience 2010 conference abstract are published. In the paper, Yakeel Quiroz, a Ph.D. student and collaborator of Lopera’s who is now at Boston University in the laboratory of Chantal Stern, reports that young carriers of the Paisa mutation activate their right anterior hippocampus more strongly than age-matched non-carriers as they encode face-name associations in an established functional MRI task (Quiroz et al., 2010). The SfN abstract (Quiroz et al., 2010) expands the finding to include the right dorsolateral prefrontal cortex and the left lateral parietal cortex. These carriers were in their thirties, with a mean age of 33.7. They perform as well as the non-carriers, but, in essence, for that their brain has to work harder. The volume of their hippocampus at that age did not differ from that of controls.
This study substantiates an earlier paper by the Swiss scientist Katrin Henke and colleagues, who had also found hippocampal hyperactivation in young pre-symptomatic carriers of a different presenilin-1 AD mutation. Henke’s study, like most prior research on individual families, was small, including but two probands (Mondadori et al., 2006). Quiroz’s paper reports on 20 carriers and 19 non-carrier family controls, bulking up the data considerably. Researchers led by Ringman also recently published fMRI data in Mexican families with a different presenilin-1 mutation. They found activation going up as carriers approached their expected age at onset (Braskie et al., 2010). Most other familial AD imaging studies are small, but that makes them no less interesting. Just last month, Swedish researchers reported that glucose metabolism went down over time in two carriers of a different presenilin-1 mutation. This happened in the posterior cingulate, the parietal, and parietotemporal cortex, and accompanied subtle cognitive decrements; see Schöll et al., 2011.
Quiroz’s results in the Colombian families speak to a debate among researchers about how brain activation changes in the decade or more before AD’s dementia phase. Findings particularly at the MCI stage have shown variable results, perhaps because change happens in biphasic curves over time, or because different regions change at different times, or because the patients in those studies were heterogeneous. More recent fMRI studies have coalesced around the notion that an early phase of hippocampal hyperactivation precedes a later hypoactivation, a biphasic curve that, to the popular imagination, suggests a brain that struggles mightily to keep up before it crashes (e.g., Dickerson et al., 2005). MCI studies support that in the sense that early stage, mildly impaired people tend to show hyperactivation, whereas more severely impaired MCI patients show hypoactivation (Celone et al., 2006). Autosomal-dominant families can help clarify this issue because they are less heterogeneous and tend to yield more consistent results.
Taken together, this means that by Paisa mutation carriers’ early thirties, some 15 years before they meet the traditional dementia diagnosis, scientists at present have three types of test in hand that distinguish carriers from non-carriers. They are the deficit on a single established cognitive test as reported in Lancet Neurology, the new binding test reported in Brain, and the functional MRI measure reported in Annals of Neurology. All these changes can be measured at what Lopera calls the “asymptomatic pre-MCI” stage, suggesting that it makes sense to start examining individuals at high risk for AD as early as 20 years before the clinical start of the disease.
Ongoing research is doing exactly that, and more. Quiroz is already imaging the brains of children because she saw some signals in teenagers, and fMRI is not invasive. API researchers and collaborators are currently analyzing CSF samples drawn from young adults in their thirties and twenties. For each marker, the scientists compare carriers and non-carries in a given age range and, if they see a difference, push back to the next-younger age range, Lopera said. Collectively, their ambition is to capture the natural trajectory of the disease in its entirety. “During this year, we plan to obtain all these biomarkers in carriers and non-carriers in all the age ranges,” Eric Reiman of the Banner Alzheimer’s Institute in Phoenix, Arizona, said at the API conference in Washington on 7 January 2011.
Don’t Count Out Old Faithful
A geyser it’s not, but the ADAS-Cog has been a trusty instrument to measure cognition in trial after trial of Alzheimer’s disease since the long-gone days of success with the cholinesterase inhibitors. Scientists especially in industry tend to use tools the FDA knows and has found adequate for drug approval before, but they agree that the ADAS-Cog is too crude to pick out those subtlest of changes by which an insidious disease like Alzheimer’s creeps up on a person over the course of many years. Likewise, the CERAD is used widely to gather standardized cognitive information harmonized through the National Alzheimer’s Coordinating Center, but it, also, is considered too insensitive to grasp the slippage from normal to mildly impaired cognition.
Or is it? Perhaps these instruments could be tuned to this purpose? This, in essence, is what Langbaum of the Banner and her colleagues did as part of their prep work for API trials. At the first API advisory meeting in October 2009, Langbaum had shown estimates of statistical power and group sizes for treatment trials that were based on data from the Banner scientists’ own research cohorts. She got advice to use more and larger cohorts and a greater range of measures, and did exactly that. “We wanted to identify which combination of cognitive assessments would most sensitively detect a person’s trajectory of change prior to an AD diagnosis,” Langbaum said. Then she would use that combo to calculate power estimates for preclinical trials.
To do that, Langbaum teamed up with Hendrix, an independent biostatistician. Hendrix had analyzed ADAS-Cog results in MCI and AD drug trials with an approach she developed, called mean-to-standard deviation ratio (MSDR). She found that some components of the ADAS-Cog actually diluted the overall result in early stage cohorts, largely because they varied greatly from person to person but changed little over time. The researchers removed these “noisy” tests and kept only the ones that were most similar among people and changed the most from year to year. That cut the needed sample size for a given trial in half. “In this case, less is more,” Langbaum said.
The researchers, notably Napatkamon (Yui) Ayutyanont, a statistician at Banner, then applied this MSDR analysis to every single test given to members of the 14-year Antioquia cohort that formed the basis of Acosta-Baena et al., 2011. She also applied it to assessments included in the cohort studies at the Rush Alzheimer’s Disease Center of Chicago’s Rush University led by David Bennett. These large studies do not use identical batteries; for example, the Antioquia study uses a modified CERAD, but Langbaum said many individual tests within those batteries are very similar or target the same cognitive domains. The scientists focused the MSDR analysis on people who changed from cognitively normal to mildly impaired, as well as comparing carriers to non-carriers (PS1, E4). In this way, they identified an optimal combination of five tests for this transition, which they will formally present at ICAD this July. The combination was similar for the Antioquia and the Rush cohorts, i.e., for a genetic and a sporadic cohort.
“This set of tests gives us an opportunity to detect cognitive decline using smaller sample sizes than we previously thought,” Langbaum said. The set provides better power to detect a treatment effect within two to three years, Reiman added.
Finally, also at the D.C. meeting, Paul Aisen of the University of California, San Diego, noted work on two further cohorts of normal elders who also can be distinguished cognitively as being on the way toward AD. For one, the 200 controls who enrolled in ADNI turned out to contain some 40 percent who had brain amyloid, and this subgroup not only had more brain atrophy over the period of observation, but they also declined slightly even on the non-optimized cognitive instruments in ADNI. For another, a separate normal aging cohort studied by David Salmon at UCSD also spotted this effect. Salmon had no amyloid CSF or PET data, but he did know the ApoE genotype of the study participants. Taking ApoE4 as a proxy for brain amyloid, he, too, found that the E4-carriers declined on delayed recall and some other tests. “This supports the idea that we can use a cognitive outcome measure in a secondary prevention study in cognitively normal individuals,” Aisen said.
Industry scientists called it a real advance for very early stage trials to have subtle cognitive markers. Viewed in isolation, such subtle cognitive changes would be considered clinically meaningless; however, the 7 January 2011 meeting of the API group featured strong consensus that in the context of all that is known about preclinical AD, these early cognitive markers will help bridge the gap between an initial biomarker response to a therapy and an eventual global outcome in patients who are years away from even an MCI or prodromal AD diagnosis.
Together, research on these tests, old and new, serves as groundwork for drug trials in this population. These, in turn, may help the design of future preclinical treatment trials in sporadic AD if indeed these markers can be used to identify people with the same cognitive and biomarker changes. The families, Lopera, and all API scientists hope that the first such trials will get underway in 2012. For more on API progress, read Part 4 of this series.—Gabrielle Strobel
Scientists and Regulators Discuss Preclinical AD Trials
On 7 January 2011, the leaders of the Alzheimer’s Prevention Initiative convened scientists at the U.S. and European medicines regulatory agencies, in industry, and academia, with statisticians and public and private funders in Washington, D.C. Their goal was to push an ongoing conversation with industry toward specifics of what sorts of trials to run, and for industry scientists and funders to hear some regulatory feedback right on the spot. Eric Reiman, Pierre Tariot, and Jessica Langbaum of the Banner Alzheimer’s Institute are leading the API team. Together with related proposals coming from the Dominantly Inherited Alzheimer Network (DIAN) and the Alzheimer’s Disease Cooperative Study (ADCS), the collective push is for therapeutic trials to start within the next two years in three different types of patients.
First, both API and DIAN are proposing studies in carriers of autosomal-dominant Alzheimer’s disease mutations, using their non-carrying relatives as controls. API researchers would like to set up a system where a given carrier gets a candidate drug for a set period of time, then undergoes evaluation of whether the drug had a benefit, and either stays on the drug if it did or moves on to a different candidate drug if it did not. Led by Randy Bateman of Washington University, St. Louis, Missouri, DIAN’s trialists are envisioning small, short studies of drug pharmacokinetics and dynamics preceding a larger efficacy trial. Second, API is proposing drug studies in people who carry two copies of the ApoE4 risk gene and have aged to within a few years of being highly likely to develop AD symptoms. Third, Paul Aisen of the ADCS is proposing a secondary prevention trial in cognitively normal people in their seventies, who are selected not genetically but by dint of having brain amyloid. In toto, these three sets of preclinical patient groups span the spectrum from rare deterministic forms to late-onset sporadic forms of AD in the general population. If results from these three groups hang together, the totality of evidence could potentially help sway regulators, even if a given trial alone is insufficient for approval, the scientists hope.
Overall, both regulators at the meeting, Rusty Katz of the U.S. Food and Drug Administration and Cristina Sampaio of the European Medicines Agency, expressed clear support for such trials. This was a big shift in the perception of many at the meeting. “You should get an award for your talks,” William Potter, formerly of Merck and now an independent consultant, told the regulators afterwards. “Industry should take notice that regulatory is not the holdup here.”
It is difficult—and quite theoretical—to design a trial without a specific drug in mind (see upcoming Part 6 of this series). A particular conundrum is that “because of the inherent lag between biomarker and clinical outcome, we do not know what outcome to pick for the trials,” Tariot said. On this problem, the regulators took a “bring ’em on” approach. They recommended that, rather than pre-specify an outcome based on thin data and then hinging the trial’s success on that guesstimate, researchers should have the trials measure a range of biomarkers and determine which is the most informative about the drug, and which, if any, is most clinically relevant to the patient.
Both Katz and Sampaio said about the proposals that the agencies are likely to take a different approach to each of the three patient populations, even though evidence from one type of trial (e.g., an ApoE4 trial) is highly welcome as additional information in the consideration of another (i.e., an autosomal-dominant Alzheimer’s disease [ADAD] trial). Regarding the DIAN and Colombia trials, Katz said that ADAD may be a valid indication by itself. Sampaio recommended that sponsors seriously consider orphan drug designation for this indication as a means of obtaining repeated and free protocol assistance along the way. “You have nothing to lose by doing that,” Sampaio said. Moreover, because of the scarcity of patients with this form of ADAD, a single pivotal trial may be enough to support approval if it comes with confirmatory evidence from outside that particular study, Katz said, repeating advice he gave at a prior DIAN meeting in London (see ARF related news story). Usually, the FDA and EMA require at least two trials. In addition, an ADAD drug need not be perfectly safe. “There is a view that a drug to treat asymptomatic patients must be extremely safe. If we had a drug that delayed the onset of inherited AD for a significant time, then that would be a huge advance. For such a drug, we could tolerate significant toxicities. We would expect the usual toxicity studies, not much more,” Katz said.
AD caused by ApoE4 is different in the regulator’s eye. Unlike presenilin or APP mutation carriers, not all ApoE4 carriers develop AD. For this reason regulators in the U.S. and Europe would set the safety bar higher for a secondary prevention drug in this group. Moreover, they do not view ApoE4 homozygote AD as a valid indication. They would not automatically extrapolate results from ApoE4 homozygote trials to all AD and approve a drug for sporadic preclinical AD based solely on ApoE4 homozygote trials. The API scientists might be asked to assess the same drug in other ApoE genotypes as well; as before, corroborating data on the same drug from any of the other populations would be welcome, Katz said.
With regard to the proposed ADCS trial of amyloid-positive elders, Sampaio encouraged Aisen. “You must do it. It is extremely important, and you should consider adaptive designs,” she said (see Part 5). At the same time, she called this trial an “academic adventure,” indicating that the current uncertainties about which outcome to use at the very early stage of sporadic AD would preclude approval for a secondary prevention drug in this population in the next five years. “I foresee getting approval in Europe in that timeframe only for ADAD. However, the trials you propose in all three populations will really give us the biomarker data we need for subsequent registration trials,” Sampaio summed up. This did not sit well with pharma scientists, who said their companies need registration trials in order to bite. This prompted discussion of public-private funding models for such trials.
Both regulators agreed that trials in a prodromal population—be it genetic or sporadic—who have even a subtle cognitive deficit that could be measured will be easier to evaluate than trials in the stage prior, where people have a genetic or biomarker risk but are truly asymptomatic. In the former, a change in a cognitive test may be sufficient clinical evidence for approval, Katz said, qualifying “‘MAY’ stands in upper case here. We’d want some ancillary data from another setting, some other cohort.” This is a big change from the previous regulatory stance, which required a cognitive plus a global clinical change. A global change may be impossible to measure at the prodromal stage; hence, a cognitive effect plus a biomarker change might be an adequate basis for approval with a disease-modifying claim, Katz said. What about the truly asymptomatic? “At this time we would not approve a treatment on the basis of an effect of a surrogate marker alone, though eventually this is likely to be the approach in patients without any pathology present,” Katz said.
One final note on a question that nags pharma companies: What if a drug causes a serious side effect in an autosomal-dominant Alzheimer’s disease patient? Would that endanger trials with the drug in late-onset AD, i.e., put the company’s investment at risk? As when often faced with a simple question, the regulators replied with an “it depends.” If the side effect seems to be due to the drug, i.e., liver failure, then it would cloud future development of that drug for LOAD and indeed any other disease, Katz said. If the side effect appears linked to ADAD, then it would not.
What does all this amount to? The regulators want these trials to happen. They offer advice on the designs. They are holding out the prospect of approval based on a single adequate trial with a biomarker and a cognitive effect, though only for ADAD at this point. That is a much more encouraging note than the agencies sounded a few years ago. “Even if the proposed studies do not, in themselves, lead to an approved indication, we hope that they will provide the evidence needed to allow for an accelerated approval pathway using biomarker endpoints,” Reiman said. And a researcher from a pharma company with late-stage AD drugs added, “I thought the regulatory pathway was the problem, but we heard a lot today to clarify that. That’s progress.”—Gabrielle Strobel.
As discouragement about a decade of negative clinical trials in Alzheimer’s disease is spreading through industry and academia alike, AD researchers are getting curious about an innovative type of trial design that is showing success in cancer and in medical device development. Called adaptive trial, it rests on Bayesian probability statistics and works quite differently from the traditional trials with which the field is familiar. Adaptive trials grabbed the limelight at a scientific and regulatory meeting of the Alzheimer’s Prevention Initiative held on 7 January 2011 in Washington, D.C. The API is a concerted, increasingly broad-based drive by researchers in Arizona and the South American nation of Colombia to get secondary prevention trials up and running in people who face a high risk of Alzheimer’s because they carry either an autosomal-dominant AD mutation or ApoE4.
Besides news on API preparations on the recruitment (see Part 2 of this series), scientific (Part 3), and regulatory fronts (Part 4), the D.C. meeting featured increasingly concrete discussions on how to design the trials. The stakes are high because treating AD years prior to dementia pushes researchers into uncharted territory with what is considered to be an especially vulnerable population. Donald Berry shook up the conversation. He advocated a type of trial that may seem radical to a field using mostly traditional randomized controlled trials (RCTs) based on what is called frequentist statistics. Besides being a statistician at the University of Texas MD Anderson Cancer Center in Houston, Berry runs a business designing adaptive trials for companies. Berry introduced adaptive trials to an audience comprising AD scientists and statisticians in academia, industry, at regulatory agencies, and public and private funders. He urged the API to consider adaptive designs because, by their very nature, they can make a virtue of the uncertainties of secondary prevention trials that can hobble conventional designs. Rather than forcing the investigator to “guesstimate” parameters they understand poorly and then hinging success or failure on the guesstimate, an adaptive trial flexibly explores that parameter while the trial unfolds. In this way, it is more likely to deliver an answer with fewer patients, Berry argued.
In broad terms, Janet Woodcock of the Food and Drug Administration (FDA) had for years called on trialists to use adaptive designs to boost the success rate and control costs of Phase 3 trials, and the FDA issued guidelines to help the transition. Calls for adaptive trial designs come up in the context of the FDA’s Critical Path Initiative. At the API meeting, regulators took the same stance. Rusty Katz of the FDA and Cristina Sampaio of the European Medicines Agency (EMA) urged the API and ADCS to venture into this new territory.
Adaptive trials are increasingly used in drug and device development, particularly in cancer, but also in migraine, stroke, diabetes, and other conditions, Berry said. “Some companies have hired whole teams; others are getting their feet wet to make sure if the train really leaves the station, they won’t miss it,” Berry said, adding that, to date, the FDA has approved one drug, the pravastatin-aspirin combination pill Pravigard, based on a wholly Bayesian efficacy analysis.
Berry claimed that an adaptive trial not only answers the question at hand faster, with fewer patients, and cheaper than a traditional trial would, but that it also gives the trial participants better medical care along the way. Typically, such trials adapt what doses or treatment arms patients get randomized to, or when to declare success or futility.
Learn as You Go
So what are adaptive trials, exactly? Starting from the underlying statistics, the main difference is that traditional RCTs regard parameters as fixed, whereas adaptive trials view them in terms of changing probability distributions. Adaptive trials measure all uncertainties by probability. Everything that is unknown has a probability distribution, and every probability is calculated conditionally on known values. As results roll in, those values go into the computer model and the numbers get re-crunched. That means incoming trial data serve to better simulate the probability of success if the trial keeps going as is, or if it changes a given parameter. Trialists then adapt that parameter to match a higher probability of success. In essence, Bayesian trials continually incorporate the latest trial data, recalculate probabilities to update knowledge, and in this way, inform ongoing decisions by the trial leaders about how to tweak the design of the trial or when to end it. “The frequentist approach typically forces you to set all assumptions, lock them in, and run with it to the end. The Bayesian approach says we can revise what the assumptions should be by monitoring them, and as the trial accrues data, you may have more accurate evidence,” said Pierre Tariot of the Banner Alzheimer’s Institute in Phoenix, Arizona.
What does this mean in practice? For example, in a trial of adjuvant chemotherapy for early-stage breast cancer in older women, the National Cancer Institute had originally required 1,800 patients; however, an adaptive design cut that number down to 600 (Muss et al., 2009). A recent trial comparing treatment options in atrial fibrillation answered the question with 167 patients and was published in the Journal of the American Medical Association (Wilber et al., 2010).
In Alzheimer’s research, finding the right dose in Phase 2, and using fewer participants, are two goals adaptive trials could accomplish, Berry claimed. Several AD scientists at the API meeting, including William Potter, who retired from Merck, had cautioned that finding the right dose was both critically important and a highly uncertain process in preclinical patients. In practice, dose finding often involves little more than guesswork, Berry charged, and by Phase 3, patient numbers in the thousands are routine. “Typically, in a dose-finding trial you administer maybe six doses. At the end, you find that all the action was between two doses where have you relatively few patients, and most patients were on doses that had no effect or were too high,” Berry said.
As an example of how to do things better, Berry cited an adaptive trial by Abbott reported at the International Society for CNS Clinical Trials and Methodology conference in San Diego in 2009. It started out with five patients on each dose, and as results rolled in, it randomized more patients to the higher doses that appeared to elicit a response and fewer to the low doses that proved early on to be ineffective. In this case, Abbott scientists declared futility, stopped the trial, and abandoned the drug, but the point is they were able to do that having used 320 patients instead of the 700 that were initially projected, Berry said. The drug flopped, but the trial was informative. Bayesian trials recruit fairly slowly to allow time to learn from incoming information and to react to it. “If you are all done enrolling before you get any information, you cannot adapt,” Berry said.
Besides finding the right dose with the minimum number of patients, adaptive trials can compare several drug candidates in one trial and help scientists decide which one to pick for Phase 3. This can be done by measuring biomarker responses to a given therapy and finding the therapy that has the highest chance of subsequently showing a clinical benefit. These twin goals of comparing drugs and using biomarkers to move a drug from Phase 2 to Phase 3 touch a nerve with AD trialists. They have a wealth of experimental drugs in their pipeline but no expeditious way of evaluating in Phase 2 which one to bet on for expensive Phase 3 registration trials. In particular, trials in asymptomatic mutation carriers will need to do this based largely on drug effects on biomarkers. Because scientists don’t know for certain how a biomarker change relates to any future clinical benefit, the fixed parameters required in frequentist trials make such RCTs inflexible and risky, Berry said. Adaptive trials could start out with, for example, control, two drugs, even a combination arm, and then drop the less effective arms. They can also test a therapy effect on a range of biomarkers initially and then drop those markers that do not respond.
An adaptive trial can accommodate up to 10 treatment arms, Berry said. Perhaps the most innovative example of that—and of data sharing in the highly competitive world of pharmaceutical drug development—is the multicenter Phase 2 breast cancer trial I-SPY 2. It is managed by the Biomarkers Consortium, a public-private partnership led by the Foundation of the NIH (FNIH). Berry co-designed the trial, and the FNIH worked out a regulatory path for participating drug companies with the FDA. I-SPY 2 started out with five different investigational drugs but intends to test up to a dozen (Patlak, 2010).
I-SPY 2 is more like a screening process than a trial, Berry said. After being adaptively evaluated for biomarker responses and a clinical outcome, a given investigational drug either graduates to a larger, specific Phase 3 trial if it performs well, or is declared futile if it fails to best standard therapy or causes a serious side effect. When a drug leaves the trial for either of these reasons, a new one enters. Drugs from Abbott, Amgen, Pfizer, and other companies are being evaluated in this single adaptive trial. “This is the most amazing piece to me,” Berry said. “Ten years ago, I’d go to one pharma company and they said ‘this sounds like good idea but I don’t want you comparing my drug in the same trial to my competitor’s.’ That is different now,” Berry said.
Given its own litany of failure and millions of dollars lost, why has the AD clinical trial research community not embraced adaptive designs? Part of the reason is technical. Adaptive designs require statisticians trained in Bayesian methods, plus massive computing power. Errors can happen, especially early on when statisticians recalculate the likelihood of success based on incoming data on the first, small numbers of patients. The FDA’s Katz said that with adaptive trials, type 1 errors, where the null hypothesis is rejected even though it is, in fact, true, are a concern. Put simply, the fear is that adaptive trials trade scientific rigor for nimbleness. In AD in particular, the endpoints that matter to the patients are thought to emerge long after a person’s initial response to the new drug. Finally, researchers don’t know enough yet about preclinical biomarkers to build the simulation models that underpin adaptive trials, said Tariot, “We know what to expect at baseline and over time for certain biomarkers in certain clinical groups, such as ApoE4 carriers; we know very little about these markers in PS1 carriers. And response to treatment is speculative in any case. Therefore, it is incumbent on us to design efficient trials with these humbling limitations acknowledged.”
Some industry scientists believe that regulators frown on adaptive trials. The opposite was the case at the API meeting. Both Katz and Sampaio spoke personally, not formally, on behalf of their respective agencies. That said, they encouraged API scientists to try adaptive designs, especially to determine the right dose and to learn what the best endpoints might be for preclinical treatment/secondary prevention trials. API leader Eric Reiman asked regulators how much flexibility the group had with regard to pre-specifying endpoints versus determining them adaptively. Their advice came down to, “The less you know for sure, the more you should adapt.” Here are excerpts from the discussion.
Sampaio: I see a lot of potential in the use of adaptive designs. You face many uncertainties, and in that situation, adaptive designs are good. If you know everything, you do not need to be adaptive. You can adapt almost every variable, though not in one and the same trial.
EMA is open to see trials with adaptive designs. Some adaptations are innocuous, others are troublesome. Adaptation of the primary endpoint is the single one the EMA usually disapproves of; we have issued guidance on that. But ignore the guidance in this case. If we always stick to guidance, we will not open new avenues. Ignoring what was written was what allowed the Portuguese to open the seas for exploration. With the trials you are proposing, you have to write a new story.
This is an extremely difficult field. You could risk doing an adaptive design even on an endpoint because you really do not know yet what the endpoint should be in asymptomatic trials. Each trial proposed today—the extremely important Colombian autosomal-dominant Alzheimer’s disease (ADAD) trial, the ApoE4 trial, the ADCS biomarker trial—is a different setting. But for each, the choice of the endpoint is the most uncertain issue. If you have the guts, that should be your adaptation.
I have thought a lot about the uncertainty regarding what is the best endpoint. Among four or five candidate endpoints, it really is guesswork these days. So why not assess them all in a trial, model them based on early data, and then find the best one? You can incorporate four or five outcomes into one adaptive study.
This may not be your single pivotal trial. It would more likely be an exploratory one that ensures the most learning.
Katz: The FDA has been encouraging more creative, adaptive Phase 2 or even Phase 2/3 trials for some time. Even so, I see very few coming across my desk.
On the dilemma of how to pick a primary outcome in patients who have no symptoms, we would like to see studies include many surrogates. Although we usually require prospective designation of key secondary outcomes, this may be a case where we have to assess the totality of the data until a surrogate emerges as the critical one. The talk on adaptive designs was pertinent here. You can start with an array of outcomes, and during the trial see which ones are responding.
The idea of using an early biomarker to predict outcome, or to identify likely responder populations, or to determine future study conduct is very intriguing. We encourage a protocol like that. It will take a lot of thought, but the FDA stands ready to entertain adaptive proposals.
In discussion, industry scientists expressed interest for API to adopt something similar to the I-SPY concept, and encouraged Berry to develop a proposal. Others pointed to how complex that would be legally, computationally, and practically. William Potter said that the FNIH biomarkers consortium could pursue the idea much like it had supported share research in ADNI and I-SPY 2. Below are some excerpts.
Paul Aisen, UC San Diego/ADCS: To play Devil’s advocate: in AD, we design a trial to give us an answer at the end of the trial with just enough patients as we need to get the answer. With adaptive designs, aren’t you taking a shortcut? You are making decisions about dropping arms, for example, before you have reached the number of subjects that you need to make that decision. There is a significant risk of making mistakes.
Berry: Frequentist trial designs force you to make so many thinly supported assumptions—especially on dose and sample size—that making mistakes has become the status quo. In AD, many frequentist trials ended with inconclusive results.
Katz: I agree about dose finding. Sometimes a company picks a dose seemingly randomly, and if they get lucky and the dose works, we approve. But in this case, where asymptomatic people take a drug a long time, it really behooves a company to find that minimally necessary dose a lot better than we often see.
Laurel Beckett, UC Davis/ADNI: Both patient burden and cost go up when we use biomarkers. Adaptive trials are the direction we need to look because they allow us to say: Let’s stop burdening the patient with this; we can already see it will not work. Or we can add patient visits if we see it will work.
David Bennett, Rush University, Chicago: A well-designed adaptive trial could take advantage of the heterogeneity of the sporadic AD group. I worry about populations that go into a trial. If you do a study in E4 homozygotes and it fails, then do you repeat the study in E4 heterozygotes anyway because that might be the subset that responds? Can an adaptive design look at heterogeneous populations?
Berry: Yes. We tend to define narrowly who enters a trial, and then when the drug is approved, everyone gets it and that leads to problems with lack of response and unanticipated side effects in Phase 4. With adaptive trials, you can learn how more different types of people respond. So for sporadic AD, I recommend to start out with a broad population and then home in where you see an effect.
Lon Schneider, University of Southern California, Los Angeles: This resonates with me. AD is a heterogeneous illness. We give that lip service, but then treat it like a homogeneous one. Doing good trials in AD is hugely complex. I want to see something like I-SPY in AD that includes and explores the heterogeneity.—Gabrielle Strobel.
Time to Open the Kimono—Which Drugs in Preclinical Trials?
At the last of a series of preparatory meetings by the Alzheimer’s Prevention Initiative, held on 7 January 2011 in Washington, D.C., API scientists impressed the audience with the work the team had done over the past year. They have the patients; they are gathering the biomarker data; they are finding suitable cognitive tests. The regulators expressed interest in the proposed trials. Adaptive designs were discussed. Beyond that, however, the scientists will come to a standstill without knowing which therapies the biopharma industry will lay on the table for these trials. “We are in striking distance of concrete designs. It hinges on specific therapies,” said Pierre Tariot of the API. “Now the field is stuck at the drug choice question,” agreed Michael Grundman of Global R&D Partners.
So, what about it? As at the previous API meeting held in Phoenix in 2010, industry scientists were coy about the topic, and no drug name came up the entire day. Differently from that meeting, though, the biopharma contingent took some flak for that stance. In particular, William Potter, formerly of Merck but now a consultant for the Foundation of the National Institutes of Health (FNIH) and other groups, pressed his colleagues. “Let us be more transparent. I am surprised that companies are not sharing more here. We can at least discuss criteria for testing and choosing drugs for these trials openly.” Other industry scientists agreed that ways of assessing and presenting data could be defined pre-competitively without one company seeing another’s raw data.
When biopharma scientists cited resistance among their senior management to sharing data and advancing candidate drugs for preclinical populations, they were asked to stop hiding behind senior management. “I do not understand our throwing up that our immutable senior management is to blame. It is not true. If we believe sharing and collaboration is important, then we have to take up this fight internally,” said Potter. And this from Maria Carrillo of the Alzheimer’s Association, “We need to stop talking about what can’t be done and to start talking about what can be done. Be as open as you can and bring senior management to these discussions.” Collectively, the group knows sharing initiatives are possible. For example, the C-Path Institute’s Coalition Against Major Diseases has developed a shared trials database, and a similar ADCS/FNIH/Alzheimer’s Association project exists as well.
Some progress has been made. Since its own regulatory meeting in London last October (see ARF related news story), Dominantly Inherited Alzheimer Network (DIAN), whose own enrollment stands at about 150, has received 10 non-binding therapy nomination packages from pharma companies. In Washington, D.C., Randy Bateman of Washington University, St. Louis, told the audience that those 10 compounds are not discontinued has-beens, as some skeptics had predicted early on. On the contrary, Bateman, said, they are the lead therapeutic candidates in the field. “That there is this amount of support from the companies to offer up their best compounds for these treatment trials is very hopeful for DIAN, for the Alzheimer’s Prevention Initiative (API), and for the Alzheimer's Disease Cooperative Study (ADCS),” Bateman said. For its part, the API is talking individually with drug companies.
In the process, though, both API and DIAN—small operations run by teams of academic scientists and their administrative staff—have been burdened by having to execute dozens of confidentiality agreements. These tie up resources these groups want to put to better use. In discussion, suggestions came up for an independent group, such as CAMD or FNIH, to lend resources and expertise. CAMD has a track record in getting companies to share trial data and to adhere to, or even convert to, a shared data standard; FNIH’s Biomarker Consortium manages the I-SPY 2 trial that could serve as a model. The idea of data sharing generated a buzz among researchers who noted that small populations such as the one in DIAN afford few opportunities to repeat tests, as well as others who want to move the preclinical trials project toward the I-SPY model.
“I-SPY is very exciting to me. Having several treatments in parallel is fascinating. The issue for us now is that 10 companies have submitted packages to DIAN, and companies are talking with API. Unless we know who they are, how are we going to move toward I-SPY? Let’s do this offline. Guys, you know my e-mail address,” said one senior pharmaceutical company scientist (name withheld).
Concluding the meeting, Eric Reiman of the Banner Alzheimer’s Center in Phoenix, Arizona, said, “Imagine one of you in this room had a drug to stop the development of a fatal disease and we did not know it. Now is the time when we have a unique opportunity to advance the evaluation of a range of pre-symptomatic compounds in the most rigorous and efficacious way. We are determined to move forward. We are heartened by the regulatory feedback. Now we look forward to engaging you.”—Gabrielle Strobel.










Comments
No Available Comments
Make a Comment
To make a comment you must login or register.