The Lou Ruvo Center for Brain Health opened in Las Vegas in 2009 as the newest site in the Cleveland Clinic network. Its mission: to advance new therapeutics and diagnostics by developing the world’s largest Alzheimer's disease clinical program to harnesses the power of a networked healthcare system. Director Jeffrey Cummings hopes to make the center a hotspot for therapeutic initiatives in other neurologic diseases as well. Toward that end, in spring 2011 the center hosted the first independent meeting of the Frontotemporal Dementia Treatment Study Group.
Las Vegas: Lou Ruvo Center Pioneers New Approach to Clinical Trials
A mere stone’s throw from shady bookstores and rundown bail bond shops stands an $80 million steel spectacle that Las Vegas mayor Oscar Goodman hopes will help revitalize this part of town. The landmark building is also poised to strengthen drug development for Alzheimer’s and other neurologic diseases, where progress has stalled amid fragmented patient care and low clinical trial recruitment. As the newest site in the Cleveland Clinic network, the Lou Ruvo Center for Brain Health is arguably breaking ground for an innovative, systems-wide approach to clinical trials.
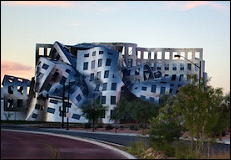
Designed by world-class architect Frank Gehry, the Cleveland Clinic Lou Ruvo Center for Brain Health opened its doors in Las Vegas in 2009. Image credit: Matt Carbone Photography
Such efforts are needed because therapeutic trials are increasingly being run by commercial groups, and are going abroad to global sites that are sometimes inexperienced or may introduce cultural and language variation into the dataset. This trend concerns Jeffrey Cummings, director of the Lou Ruvo Center, which opened its doors in the summer of 2009 and now sees some 75 patients a week for a combination of clinical care and research. “We can capture a greater proportion of trials within the U.S., and get many more patients enrolled in them, if we capitalize on the ability of healthcare systems to embrace clinical trials as a major part of their activities,” Cummings told ARF. “Our purpose is to advance new therapeutics and diagnostics for AD by developing what will be the world’s largest AD clinical program that harnesses the power of a networked healthcare system.” The new center looks to gain some national prominence with the May 1 CNN airing of Unthinkable: the Alzheimer’s Epidemic, in which talk show host Larry King and Ron Reagan, the late President’s son, will be seen visiting the new center.
Launched with funds raised by Las Vegas businessman Larry Ruvo, whose father Lou died of AD in 1994, the 65,000-square-foot center was conceived by the late Leon Thal (see ARF obituary) as an enterprising model for patient care and outside-the-box collaborative research in neurologic disease. Wanting a signature building commensurate with these lofty goals, Ruvo summoned world-class architect Frank Gehry to the task. Originally, the University of Nevada, Reno, was to provide infrastructure and run the center’s clinical operations, but a dearth of dollars dried up those plans just as Cleveland Clinic was looking to expand westward. The entrepreneurial healthcare provider swooped in to cut a deal in February 2009 (see ARF related news story), and last summer hired Cummings to head the Ruvo Center’s research and operations and to build neuroscience programs at Cleveland Clinic’s main campus and other sites in Lakewood, Ohio, and Weston, Florida. “We will simultaneously have the same trials going on with the same IRB (institutional review board) in all these and possibly other sites,” said Cummings, who formerly directed the Alzheimer’s Disease Research Center at the University of California, Los Angeles. The UCLA center now runs under the leadership of interim director John Ringman.
The Ruvo Center is focusing on patient services, and research at the Las Vegas site will be translational. “Now we are part of Cleveland Clinic,” Cummings said. “The vision had to be consistent with the new operational reality.” Cummings’ broader thinking is that the patients-first philosophy of the clinic will bolster therapeutic development because it can empower patients to help solve the diseases that afflict them by participating in clinical trials, Cummings told ARF. “We are an integrated clinical and research operation that works with patients to develop new therapeutics.”
The vast majority of dementia patients have a hard time getting adequate care, said Rachelle Doody, who directs the AD and Memory Disorders Center at Baylor College of Medicine in Houston, Texas. “Their internist doesn’t know about their dementia. Some get one set of blood work, others another. Many physicians don’t have well-developed approaches that coordinate with each other,” Doody said. Furthermore, she noted that only a tiny fraction of newly diagnosed dementia patients “even consider enrolling in a trial, because the doctor doesn’t know they exist, or doesn’t know where they are.” (For more on integration of patient care and clinical research, see Doody, 2009.)
Furthermore, at academic memory centers, patients often need to trek all over campus for their various assessments. With neuropsychiatric testing in the memory center, lab work in a separate building, and brain imaging done across campus in the radiology department, getting comprehensive care can turn into a drawn-out navigation exercise for the navigationally challenged and their caregivers. “In academic settings, things tend to be scattered around,” Cummings said. “Here, they are all provided within one building, including information about clinical trial opportunities.”
Spacious, semicircular hallways with brightly colored furniture remove the dreary institutional feel one commonly associates with hospitals. The space combines easy access to magnetic resonance imaging (MRI), neuropsychiatric assessments, occupational and physical therapy, social work referrals, and longitudinal care. Patients go into one set of rooms for research or into adjacent rooms for clinical care. At each visit, they answer questions on their mood, lifestyle, habits, and the like using a hand-held computer that gets passed on to a nurse who continues entering information in the exam room. Paperless systems like these are “upper-end state-of-the-art” among memory clinics, Cummings said. Incidentally, this is routine in the return of a rental car and many restaurants, showing how general healthcare is still behind in its use of digital records.
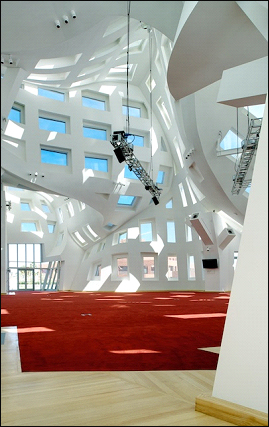
Hospitality is a high priority for the Cleveland Clinic Lou Ruvo Center for Brain Health in Las Vegas. Photos show the courtyard (top) and interior hallway (bottom). Image credits: Matt Carbone Photography
AD patients receive functional and structural MRI imaging on a 3-Tesla scanner according to the Alzheimer’s Disease Neuroimaging Initiative (ADNI) protocol regardless of whether the patients are enrolled in ADNI. This will make their MRI data comparable to the ADNI dataset. The Ruvo Center plans to purchase a positron emission tomography (PET) scanner; in the meantime, patients get their PET imaging at the Nevada Cancer Center.
Ruvo’s father dreaded running into clinic patients with advanced AD while he was still at the early stages of disease, Cummings said. Indeed, seeing where the disease inexorably leads some years down the road is frightening for many patients. For this reason, Gehry designed the four-story center so interaction between patients with mild and severe disease would be minimal, Cummings said. For the most part, patients are escorted straight into their exam rooms. The waiting area has just two chairs.
After finishing their assessments, patients and their families can lounge in “tranquility” rooms—essentially, upscale waiting areas—while the caregivers fill out paperwork and schedule future appointments. The Ruvo Center has designated counsel rooms for families to process difficult news and make decisions.
Other amenities include elevators with rotating art galleries, high-end cuisine served on custom dinnerware at the Maria Puck Café (named after the AD-stricken late mother of celebrity chef Wolfgang Puck), and fresh flowers for all patients as they leave the center. Caregivers can attend weekly Lunch & Learn programs, as well as on-site dance and theater classes. “Our goal is that the patient experience will be one of hospitality, not just a series of clinical assessments,” Cummings said. Similarly, creating a non-clinical, reassuring environment for integrative dementia care is also a hallmark of Cognitive Fitness and Innovative Therapies (CFIT), an independent center that opened in Santa Barbara, California, in 2009 (see ARF related news story; ARF Webinar). One difference is that CFIT focuses more on a holistic approach to preventive and cognitive care, whereas Lou Ruvo focuses on integrating medical care with clinical trials on site.
The approach may be paying off. A hefty 20 to 30 percent of the patients at the Lou Ruvo Center enroll in trials, and have higher retention rates, too, noted Kate Zhong in an e-mail to ARF. Zhong, a geriatric psychiatrist who formerly led global clinical trials for AD therapeutics at AstraZeneca, now directs clinical research and development at the Ruvo Center. “We have a unique system in which the referral intake and screening process are integrated into the clinical practice,” Zhong wrote. “Every patient is potentially a clinical trial candidate.”
At present, the center is the leading recruitment site for patients entering the Phase 3 trial of intravenous immunoglobulin (IVIg), a preparation of human antibodies made by Baxter BioScience. Altogether, center patients participate in 10 ongoing trials for AD or mild cognitive impairment, with another eight or so trials pending or in discussion. In addition, the facility is a site for two ongoing Parkinson’s disease studies—a Phase 3 trial of preladenant (an adenosine A2A receptor antagonist developed by Schering-Plough), and a bike exercise trial for which the Las Vegas center is the sole site.
Beyond conducting clinical trials in a patient-friendly environment, Cummings’ other goal is to make the center a focal point for discussions on novel neurotherapeutics. The number of current trials for many neurodegenerative diseases, such as the tauopathies, for example, is still deplorably small, Cummings said. On this front, the center is trying to invigorate research by bringing academic and industry scientists together with government agencies and advocacy groups to discuss how the sectors can collaborate to move frontotemporal dementia (FTD) compounds more quickly into the clinic. Just last month, the center hosted "Frontotemporal Dementia: The Next Therapeutic Frontier," the first independent meeting of the Frontotemporal Dementia Treatment Study Group. To learn all about that, see Part 2 and Part 3.—Esther Landhuis.
Las Vegas: Are Frontotemporal Dementia Models Fit for Pharma?
Huddled around conference tables in an $80-million building designed by the star architect Frank Gehry, some 65 representatives from academia, industry, advocacy groups, and government agencies met 25-26 March 2011 for dialogue whose concentrated intensity evoked the neon glare of the Las Vegas strip just a few miles south. Their discussions tried to illuminate a path toward treatments for frontotemporal dementia (FTD). FTDs afflict 200 times fewer people than does Alzheimer’s disease, but lead to death sooner and are as common as AD in people 65 or younger. Many FTD patients are still misdiagnosed as having AD or a psychiatric disorder, and frontotemporal dementias have as yet no specific therapies.
However, recent research advances have ignited the field—so much so that last year a handful of academic and pharmaceutical scientists launched a study group to speed drug discovery for these rare disorders. The FTD Treatment Study Group (FTSG) met for the first time in April 2010 at the annual meeting of the American Academy of Neurology in Toronto, then again in October at the 7th International Conference on Frontotemporal Dementias in Indianapolis, Indiana (see ARF related news series). Last month, the fledgling organization held its first independent meeting, “Frontotemporal Dementia: The Next Therapeutic Frontier,” in Las Vegas.
The Frontotemporal Dementia Treatment Study Group held its first independent meeting 25-26 March 2011 at the Cleveland Clinic Lou Ruvo Center for Brain Health, which opened in Las Vegas in 2009. Image credit: Matt Carbone Photography
The conference took place at the Cleveland Clinic Lou Ruvo Center for Brain Health, whose 18,000 curving stainless steel shingles and 199 uniquely shaped windows arguably make it a Lady Gaga among neurodegenerative disease facilities. “You’re in one of the greatest buildings in the world,” director Jeffrey Cummings told attendees. “At this meeting, we should have thoughts commensurate with this building.” To facilitate outré thinking, Cummings and others on the FTSG steering committee packed the one-and-a-half-day agenda with talks on preclinical animal models for FTD and lessons from collaborative therapeutic initiatives in other neurodegenerative disorders, and spiced up discussion with proposals ranging from a Web-based registry of FTD models to an independent clearinghouse for deciding which compounds should get tested in which models. The organizers are summarizing conference proceedings in a position paper to be published in a peer-reviewed journal. In anticipation of this detailed, formally referenced article, this story briefly recaps the key science reported in Las Vegas. See Part 3 for the collaborative drug discovery proposals and pharma’s response to them, and Part 1 for a broader vista on the Lou Ruvo Center and its mission to rejuvenate clinical studies of neurodegenerative disease.
Along with Cummings, the FTSG steering committee consists of Susan Dickinson, Association for Frontotemporal Degeneration; Howard Feldman, Bristol-Myers Squibb; Howard Fillit, Alzheimer’s Drug Discovery Foundation; Michael Gold, Allon Therapeutics; and Megan Grether, Bluefield Project to Cure Frontotemporal Dementia. Adam Boxer, University of California, San Francisco, chairs the committee and organized the scientific component of the recent meeting.
Nine pharmaceutical companies sent representatives to Las Vegas. Boxer explained why their industry should find it in their interest to invest in FTD. Beyond the incentives that come with FTD’s orphan drug status and new diagnostic criteria, frontotemporal dementias progress rapidly—much quicker than AD, whose slow progression has made trials on this disease long and costly. “Theoretically, one could do a shorter trial and have greater power to detect an effect,” Boxer said. People with FTD also tend to be younger and have fewer comorbidities than AD patients. Furthermore, Boxer noted, some FTD syndromes have a clearer link to specific molecular pathology than in AD, where a mixture of amyloid, tau, synuclein, and even TDP-43 pathology may contribute to the clinical phenotype. In this regard, FTD with parkinsonism linked to chromosome 17 (FTDP-17) and progressive supranuclear palsy (PSP)—both pure tauopathies—rank among the top FTD treatment candidates, Boxer said. Another is progranulin-related FTD, which looked therapeutically promising in a subsequent presentation by Fen-Biao Gao, University of Massachusetts Medical School in Worcester.
Speaking on behalf of Feldman, who could not attend, Gary Tong of Bristol-Myers Squibb reminded attendees of the abysmal odds faced by CNS drugs coming through the clinical development pipeline. Of compounds tested in Phase 1 studies, 1 or 2 percent eventually reach market. Among those surviving to Phase 3, a mere 15 percent make it all the way. Drug development for FTD is particularly difficult, in part because of the heterogeneity of clinical syndromes. In addition, Tong said, outcome measures are not optimized, and cellular and animal models are insufficiently validated. “How do we know these models will translate to clinical efficacy?” he asked. “This is a major issue.”
That concern also surfaced in Gao’s talk. A big problem with many FTD models is that they rely on overexpression of proteins in order to produce disease phenotypes, Gao said. He and others skirt this problem by generating patient-specific induced pluripotent stem cells (see ARF iPS series). Collaborating with Bruce Miller and Robert Farese of UCSF, Gao reported collecting skin biopsies from 29 FTD patients and 17 controls. The team used the samples to generate around 200 iPS cell lines, a few of which have been confirmed pluripotent. Some of the iPS lines show reduced progranulin, the gene behind 5 to 10 percent of FTD cases. Scientists can use these cells to screen for compounds that enhance progranulin expression, including an FDA-approved histone deacetylase inhibitor (suberoylanilide hydroxamic, or SAHA), as reported in a freely downloadable paper published online March 23 in the Journal of Biological Chemistry (Cenik et al., 2011).
Also in Las Vegas, Ed Burton, University of Pittsburgh, Pennsylvania, reported on his lab’s efforts to develop tauopathy models in another animal that looks promising for screening potential therapeutic compounds. This is the zebrafish. The scientists made transgenic fish expressing human tau specifically in neurons (Bai et al., 2007). These animals looked normal up until around six months, when they started having trouble breeding. The trouble stemmed from behavioral and motor defects that progressed with age. Consistent with these deficits, the transgenic fish had smaller brains, hyperphosphorylated tau, and more microglia.
While these zebrafish look promising as a tauopathy model, therapeutic studies work more easily in fish that develop pathology at larval stages. “Larvae are possible to screen on 96-well plates,” Burton said. His team has used the Gal4/UAS system to create stable tau transgenic lines with high expression levels in the brain. Researchers led by Christian Haass and Bettina Schmid at the Ludwig-Maximilians University in Munich have used a similar approach to create transgenic fish that express tau in the spinal cord (see ARF related conference story on Paquet et al., 2009).
Are these models ready for pharmaceutical application? “I think we are close with the Gal4/UAS animals,” Burton said. In preliminary studies, he and colleagues have detected 30 percent rescue of movement defects with a sample size of four fish. Computer systems can detect larval eye movements, and these reflexive behaviors can be used to validate compounds that have a motor effect. (For reviews on tauopathy zebrafish models, see Bai and Burton, 2010 and Bandmann and Burton, 2010.)
On the fly front, George Jackson and coworkers at the University of Texas Medical Branch, Galveston, uncovered 41 tau modifiers in a recent genomewide screen covering 20 percent of the Drosophila genome. As expected, GSK3β and other tau kinases appeared among the gain-of-function modifiers. The autophagy gene ATG6 (aka Beclin-1) turned up on the loss-of-function list. The researchers then did an “unbelievable number of Westerns” with the AT8 phospho-tau antibody, hoping to link modifier effects with tau phosphorylation, but, surprisingly, found no such correlation, Jackson reported. Furthermore, his team made phosphorylation-resistant tau mutants and showed they were still toxic. Perhaps phosphorylation “is not a sine qua non for tau toxicity,” Jackson said. “The data suggest that kinase inhibition may not be the best target.”
More complex models were also on the agenda at the Lou Ruvo meeting. Kathleen Zahs works with Karen Hsiao Ashe at the University of Minnesota, Minneapolis, on developing tau transgenic mice. In the group’s Tg4510 mice with regulatable forebrain expression of the FTD-linked P301L human tau mutant, they previously showed that turning off tau expression rescued memory and neurodegeneration even as the mice continued to form tangles (see ARF related news story on Santacruz et al., 2005; Ramsden et al., 2005). This suggested that soluble tau disrupts synaptic structure and function prior to neurodegeneration. The scientists’ hypothesis was proved correct in recent analyses showing that mutant tau mislocalizes to dendritic spines, causing loss of glutamate receptors and weakened synaptic signaling early in disease in the Tg4510 model (ARF related news story on Hoover et al., 2010).
Thus far, research with these mice has focused on mechanisms. In preclinical studies, it is critical to understand what aspect of disease is being modeled in any particular mouse in order to use it appropriately, Zahs said. She noted that APP transgenic mice model largely the asymptomatic phase of AD, making them well suited for prevention, but not treatment, studies. In the case of the Tg4510 mouse, “we see neurodegeneration (likely due to the mutant P301L tau) superimposed upon a developmental delay (likely due to tau overexpression), and any preclinical studies in these mice should take into account that they are not a model of pure neurodegeneration,” Zahs said.
Blair Leavitt, University of British Columbia in Vancouver, Canada, spoke about his conditional progranulin knockout mice, which he first reported at last year’s International Conference on Alzheimer’s Disease in Honolulu (see ARF related conference story). These animals show subtle, sex-specific abnormalities in social behavior, as well as defective neuronal morphology and impaired synaptic plasticity and long-term potentiation; all this happens at eight months of age and about 10 months before evidence of neuropathology in this model. These mice are “not quite ready” for testing potential therapeutics, Leavitt said, “but we are getting to a point where we are finding real and practical endpoints.” Besides being expressed in mature neurons, progranulin normally shows up in microglia (but not astrocytes) and gets upregulated in activated microglia. To explore its role in these macrophages of the brain, graduate student Terri Petkau is generating mice with a conditional progranulin deletion in microglia.
On the theme of microglial-neuronal interactions, recent work by Cleveland Clinic colleagues Bruce Lamb and Richard Ransohoff suggests that signaling through the fractalkine receptor CX3CR1 on microglia could be “an interesting pathway to consider for therapeutic interventions,” Lamb said. The scientists found that mice lacking CX3CR1 show exacerbated tau hyperphosphorylation in response to microglial activation. Similar tau changes appeared in another strain generated by introducing wild-type human tau into a mouse tau knockout. These mice had behavioral impairments that correlated with increased levels of p38 MAP kinase (ARF related news story on Bhaskar et al., 2010). In essence, the scientists believe, healthy neurons signal via this fractalkine receptor to microglia to keep them from getting activated. “If we can induce this pathway, it may have a protective effect in tauopathy models,” Lamb said.
Erik Roberson, University of Alabama at Birmingham, first outlined key challenges for modeling FTD in mice and then allayed each of these concerns with his lab’s recent data on progranulin-deficient mice made by Farese’s group at UCSF (see ARF related conference story) and mutant tau transgenic mice made by Gerard Schellenberg when he was at the University of Washington, Seattle (McMillan et al., 2008). One challenge with mouse models is that FTD involves the prefrontal cortex, a brain area that is dramatically expanded in humans compared to mice. Another is that FTD patients show dysfunctional social and emotional behaviors that seem too complex to find in rodents (see ARF related conference story). How much empathy for others, fidelity to a spouse, or financial prudence does the mouse show in the first place?
To the first point, Roberson reminded attendees that the field is shifting toward a network-based view of FTD. The disease’s primary target is not really the prefrontal cortex, but rather connectivity throughout the brain’s salience network, which includes the anterior cingulate, insula, amygdala, striatum, and brain stem areas—all of which are well represented in the mouse brain (ARF related news story on Seeley et al., 2009). This change in thinking also came up in a talk by Bruce Miller of UCSF. He stressed that brain atrophy patterns for various FTDs map to functional networks whose neurons “are not only born together and fire together, but also die together.”
On the second issue—the complexity of social and emotional behaviors in FTD—Roberson described several outcome measures that do seem to reveal rodent versions of the emotional blunting, social dysfunction, and repetitive behaviors common to FTD patients. On the former, progranulin-deficient mice show unusually high interest in inanimate objects in a sociability test, and subdued responses to aversive stimuli in a fear-conditioning test. Other measures reveal hints of social disinhibition and age-dependent repetitive behavior in tau transgenics. These mice spend considerable time exploring open, exposed arms of an elevated-plus maze—“dangerous” areas that dark-preferring wild-type mice avoid. In addition, tau transgenic mice develop facial lesions from compulsive grooming that intensifies with age. The behavioral impairments seem to correspond with anatomical abnormalities, as these animals show specific electrophysiology and morphological defects in the ventral striatum, the brain area at the root of repetitive behaviors in people with FTD.
Beyond progranulin and tau, the gene for valosin-containing protein (VCP), which is implicated in autophagy, causes some cases of familial FTD. Toward the end of his keynote address, Frank LaFerla of the University of California, Irvine, shared preliminary data on his lab’s brain-specific VCP transgenic mice. Relative to wild-type controls, these animals show spatial memory defects in the Morris water maze, as well as abnormal astrogliosis, protein ubiquitination, reduction of the autophagy marker LC3II, and accumulation of cytosolic inclusions containing TAR DNA-binding protein 43 (TDP-43).
“It’s exciting that there appear to be a number of models at different levels that are looking mature in terms of recapitulating FTD phenotype,” Boxer told ARF.—Esther Landhuis.
Santacruz K, Lewis J, Spires T, Paulson J, Kotilinek L, Ingelsson M, Guimaraes A, DeTure M, Ramsden M, McGowan E, Forster C, Yue M, Orne J, Janus C, Mariash A, Kuskowski M, Hyman B, Hutton M, Ashe KH.
Tau suppression in a neurodegenerative mouse model improves memory function.
Science. 2005 Jul 15;309(5733):476-81.
PubMed.
Las Vegas: Can Collaboration Speed Drug Discovery for FTD?
Given their complex pathophysiology and bewildering array of clinical symptoms, frontotemporal dementias (FTDs) have long stymied scientists’ attempts to model these disorders at the lab bench and to test drugs against them. However, at the "Frontotemporal Dementia: The Next Therapeutic Frontier" meeting held 25-26 March 2011 in Las Vegas, stakeholders from academia, pharma, nonprofits, and government agencies heard about a recent surge of developments that suggest the tide may be turning (see Part 2). “There are many potential approaches, and oodles and oodles of models. You really don’t know how to pick and choose,” Michael Gold of Allon Therapeutics, Vancouver, Canada, told ARF. And when it comes to testing disease-modifying compounds for disorders that are 200 times less prevalent than Alzheimer’s, companies need to be choosy about which ones they push into the clinical pipeline. “We don’t have the luxury of doing a lot of trials,” said Adam Boxer, University of California, San Francisco. “We have to be sure a compound is a good bet going into a trial.” Boxer chairs the steering committee of the FTD Treatment Study Group (FTSG), which includes Gold and four others (see Part 2). The group formed about a year ago to accelerate drug development for these disorders, and sponsored the recent conference at the Cleveland Clinic Lou Ruvo Center for Brain Health in Las Vegas.
Other rare disorders face similar predicaments, and independent nonprofit organizations have stepped in by facilitating collaboration among academia, industry, and government bodies. In Las Vegas, attendees heard about several of these initiatives and weighed in on similar efforts brewing for FTD.
The event center of the Cleveland Clinic Lou Ruvo Center for Brain Health receives natural lighting from 199 uniquely shaped windows. This space hosted the first independent meeting of the Frontotemporal Dementia Treatment Study Group, held 25-26 March 2011 in Las Vegas. Image credit: Matt Carbone Photography
With a single identified gene mutation causing the disorder, Dan van Kammen hailed Huntington’s disease as a poster child for drug development in rare diseases. Recently retired from the Cure Huntington’s Disease Initiative (CHDI) Foundation, Inc., van Kammen described how CHDI has worked with biotech and pharma companies to develop a pipeline of therapeutic targets. As a virtual biotech, CHDI has standardized HD animal models and cell assays for evaluating potential therapeutic approaches, and rallied scientists worldwide to share data and form collaborations with the shared mission of speeding HD drug development.
To make this happen, CHDI has created a website where researchers can exchange ideas and learn the latest on HD drug discovery efforts. In an effort to impart some standardization and comparability on the individualized nature of academic datasets, the foundation has developed a scorecard for assessing mechanistic data and “druggability” of some 800 molecules claimed to be involved in HD. This is annotated on the website, which is open to registered users.
More recently, CHDI worked with the Public Library of Science to launch PLoS Currents: Huntington Disease, a peer-reviewed journal that processes manuscripts rapidly and, importantly, accepts negative data that might otherwise never see the light of day. This may prevent scientists from wasting time and money on unsuccessful research paths, van Kammen noted. “Research foundations today have an important role in serving as a safe meeting ground for academia, NIH, and industry to address issues important for drug development that are unlikely to be addressed by any party alone,” van Kammen said.
Besides expressing support for those efforts, National Institute of Neurological Disorders and Stroke (NINDS) program director Margaret Sutherland discussed the induced pluripotent stem cell initiative funded by NINDS. It aims to create fibroblast iPS lines with known mutations for Huntington’s, Parkinson’s, or amyotrophic lateral sclerosis (ALS), and make the cells available to scientists through biobanking at Coriell Institute for Medical Research in Camden, New Jersey (see ARF iPS story). The iPS consortia are “an example of where government, academics, non-government organizations, and pharma can come together to work toward a common goal,” Sutherland said. “It works because it is a noncompetitive space. We all recognize similar limitations.”
Steve Perrin heads the ALS Therapy Development Institute (ALS TDI), a nonprofit organization in Cambridge, Massachusetts. There, some 30 scientists, mostly from pharma, plug away with a singular objective, that is, developing drugs to stop amyotrophic lateral sclerosis as soon as possible. In Las Vegas, Perrin discussed the importance of rigorous preclinical study design, the relative lack of which in the past he sees as the reason many drugs that look fantastic in mice later flop in human trials. He used as examples three compounds (celecoxib, minocycline, and lithium) with preclinical data published in high-tier journals that failed to translate in the clinic. All ended up in Phase 3 trials, but would have never reached human testing had the preclinical studies been held to more stringent standards, Perrin said (see also Alzforum Webinar).
Among the standards Perrin mentioned were these: making sure mice are dying of ALS instead of something else, genotyping to check the transgene copy number in transgenic animals, examining outcomes separately in male and female mice. Had such guidelines been used, none of these three compounds would have helped ALS model mice nearly as much as, for example, blocking interactions between CD40 and its ligand CD40L, a separate potential therapeutic approach identified in a recent analysis by Perrin and colleagues (ARF related news story on Lincecum et al., 2010; stay tuned for upcoming Alzforum Webinar with Perrin).
Whereas ALS TDI takes a brick-and-mortar approach to fighting ALS, the Coalition Against Major Diseases (CAMD) works in large part as a distributed organization coordinating projects for AD and PD. An initiative of the Critical Path Institute, CAMD has an online data repository with information from some 4,000 AD patients in 11 industry-sponsored clinical trials. Last November, CAMD gathered representatives from academia, industry, funding, policy, and regulatory authorities in Washington, DC, to discuss ways to reform AD drug trials (see ARF related series). In Las Vegas, Marc Cantillon, CAMD’s executive director, stressed the importance of formal legal agreements in making these collaborations work. The contracts not only compel all parties to share data, but also spell out exactly what will be done with the intellectual property generated by the joint research.
CAMD showed that “companies are willing to part with proprietary information,” Gold told ARF. “You can get big companies to contractually agree to share data with a neutral third party.” Gold challenged the Lou Ruvo audience to consider a similar arrangement for accelerating FTD drug discovery. “We are far behind the AD field in terms of how we are organized, how we share data, and how we do clinical trials. It is high time that we start to focus and customize the treatments,” he said. “The fundamental question is, How do you pick which compounds to move into clinical trials?”
Such issues are critical for tauopathies, which by virtue of their lower prevalence and heterogeneity will have much smaller markets. A smaller potential return limits companies’ willingness to invest. “With low prevalence conditions, you have multiple resource constraints,” Gold said. “If you are talking about disease-modifying compounds…these will likely entail long studies. We need to think more carefully about what molecules we move into such expensive studies, and what strength of evidence is required.”
To help the field make these decisions, Gold laid out a “collaborative competition” model, whereby only the most promising compounds would get tested in the most relevant models. “We are looking for a rational transaction that optimizes the outcome,” he said. Not long ago, such transactions were simpler because they were mostly unidirectional—Party A (academic lab) developed a model that could be used to test compounds developed by Party B (company). Nowadays, the lines are blurring as companies make models and universities try their hand at compound screening and medicinal chemistry. “Party A or B may be either a pharma company or an academic center,” Gold said. “Intellectual property issues are more convoluted.”
In the framework Gold envisions, all parties would sign a contract agreeing to share their data with an FTSG-run “clearinghouse” for FTD drug discovery that would match compounds to models based on a pre-specified scoring procedure. Gold compared this process to those used by the National Resident Matching Program to connect medical school graduates with residency programs, or by the National Collegiate Athletic Association for matching student athletes with schools. The clearinghouse would be funded by all participants, though not necessarily equally by academic labs and companies. “Everybody shares in the risk. Everybody potentially shares in the reward. We need to work together, but at the end of the day, only the best compounds should enter the clinic,” Gold said. Beyond setting licensing terms, the clearinghouse could create and administer patent pools, Gold said, and help arrange cross-licensing across multiple parties—for example, to license a model for the testing of more than one molecule.
In a subsequent presentation, Boxer showed a mock homepage for an FTD website to facilitate the data sharing that would fuel the clearinghouse. The proposed website would serve as a go-to for information on FTD, treatment development, and on the FTD Treatment Study Group. It would have pages describing the various animal and cellular models—their strengths and weaknesses, genetic tools available, targets that could be tested, studies by other investigators using the model, and so forth. In addition, Boxer said, the website would have a password-protected section where pharma scientists could contribute information on potential therapeutic compounds.
On this, the FTSG has its work cut out. Few pharma scientists spoke up during discussion of the website and clearinghouse ideas. The ones who did, as well as others who spoke with this reporter at the meeting and/or via e-mail afterward, expressed as much hesitation as excitement for these proposals. Susan Abushakra of Elan Corporation, South San Francisco, noted that, in her personal opinion, it would “need an army of lawyers” to get companies to give proprietary data to a shared website they do not control. Another industry scientist said the website is “great for academia” but “would not work with industry.”
However, some pharma companies might be willing to say they have certain data—for example, whether a compound has gone through certain stages of preclinical development, or whether it has been tested in various animal models—without disclosing precisely what the data are, suggested Gerhard Koenig of EnVivo Pharmaceuticals in Watertown, Massachusetts. “That’s one way industry may be able to contribute (to the website),” he said. Another option for industry participation might lie with compounds that are either non-druggable or have no intellectual property protection, Abushakra suggested, “These can be used as probes or tools to characterize the non-clinical models.” Gold stressed that the terms under which data are loaded onto the website would be negotiated and clear to all parties beforehand.
Several attendees articulated the concern that academic researchers are not given proper incentives to do the best drug development studies. “Negative studies don’t get published, and you don’t get rewarded for doing replicative studies that try to confirm the same thing in a variety of different models,” Boxer told ARF. Toward this end, several company directors said a joint website could hold great value as a central repository for preclinical data, both positive and negative. Blair Leavitt of the University of British Columbia, Canada, wondered whether the field needs something like a ClinicalTrials.gov for animal studies. “Negative results have to be brought out,” he said.
Beyond data sharing, a website might drive drug discovery forward by displaying the licensing terms for various models, an industry representative noted. “It would be useful if, up front, institutions with models would work with their legal licensing groups to make terms for academic and industrial use clearly available upon request, and post these on the website,” he wrote. In AD, the Jackson Laboratory’s Alzheimer’s Disease Mouse Model Resource has addressed some of these problems. Led by Mike Sasner at JAX in Bar Harbor, Maine, this project obtains and re-derives desirable mouse models in the field and makes them available for a nominal fee to other investigators. In the process, the resource has gained experience with many of the institutional licensing problems that come up.
As for the proposed clearinghouse, some were concerned it could actually slow drug development. “Committees are not the best way to make decisions in a difficult, evolving field,” one company executive suggested. “Many successful drug hypotheses have been ‘maverick’ ideas that failed to get approval by committees for funding, or support by colleagues in pharma companies. I hope the FTD Treatment Study Group will focus on facilitating vigorous debate rather than act as a gatekeeper.”
On the whole, companies found the meeting packed with new data on FTD preclinical models that could lead to increased pharma interest—but most are not jumping into the fray just yet. “We will continue to watch developments in this evolving area very closely,” wrote Greg Flesher of Avanir Pharmaceuticals, Aliso Viejo, California. “Tau therapies are exciting, but very early and high-risk programs.” A wait-and-see approach is not enough for Jeffrey Cummings, who directs the Lou Ruvo Center in Las Vegas and serves on the FTSG steering committee. “We can have meetings until the next ice age…but if our mission is to accelerate entry of compounds into clinical trials, then we need a different framework that requires exchange of proprietary information,” Cummings said.
In Las Vegas, attendees knocked heads over the pros and cons of various organizational and funding models for the FTD Treatment Study Group, including the possibility of a formal affiliation with the Association for Frontotemporal Degeneration (AFTD). Whatever solution they’ll arrive at, the group knows it wants “to stay focused on drug development for FTD, on getting molecules to the clinic,” Boxer told ARF. The next meeting of the FTD Treatment Study Group will focus on clinical trials and biomarkers, and will likely occur in conjunction with the Clinical Trials on Alzheimer’s Disease Conference, 3-5 November 2011 in San Diego.—Esther Landhuis.



Comments
No Available Comments
Make a Comment
To make a comment you must login or register.