At the Alzheimer's Disease Research Summit 2012, held 14-15 May 2012 at the National Institutes of Health, speakers cited the Dominantly Inherited Alzheimer Network (DIAN) as an example of the kind of integrated observational and treatment initiative that advances the field.
DIAN Grows, Gets Ready for Therapeutic Trials
On 14 April 2012, the Dominantly Inherited Alzheimer Network (DIAN) Pharma Consortium met in Washington, D.C., to exchange the latest information on DIAN’s preparation for therapeutic trials. On the road toward doing something unprecedented—offering preventive drug trials to carriers of Alzheimer’s disease mutations who live scattered around the world—the day marked progress on growing the network, nailing down outcome measures, first glimpses at longitudinal data, and regulatory clarifications. Here is a summary in two parts.
As of April 2012, DIAN had enrolled 242 participants, John Morris of Washington University, St. Louis, Missouri, told the audience of some 50 scientists in academia and industry. With that, the network met its original recruiting goal of 240. One hundred thirty-three of 212 (63 percent) are confirmed mutation carriers, of whom 75 are asymptomatic. In the past, there had been doubt that participants would comply with DIAN’s extensive requirements, or would stay with the six-year study. In fact, most participants complete all assessments; even the lumbar puncture rate exceeds 80 percent, and nearly all return for their repeat visits. “This is a highly dedicated group,” Morris said.
DIAN needs more participants to be able to create the statistical power of the therapeutic trials it plans to offer. Currently, DIAN is continuing to enroll toward a revised goal of 400. DIAN’s Therapeutic Trials Unit (TTU), led by Randall Bateman of Washington University, is surveying 75 additional clinical locations in the U.S., Europe, and Canada. The DIAN TTU asks the sites how many ADAD family members are in their care. It also inquires about facilities and resources, and other criteria to probe the site’s potential to join future DIAN treatment studies. This ongoing process to date has identified more than 300 additional asymptomatic individuals who may be interested in therapeutic trials once they learn about them and the trials are ready to recruit. Bateman expects that many more carriers remain to be discovered. “Studies usually focus on symptomatic individuals, not on their asymptomatic family members, but they are there,” Bateman said.
Of the more than 320 newly identified symptomatic carriers and over 330 asymptomatic carriers, about 285 asymptomatic carriers live in Denmark, Finland, France, Germany, Italy, Japan, The Netherlands, Spain, and the U.K. Intriguingly, investigators also found seven sites in Russia and Bulgaria that are in contact with ADAD families, many of them with confirmed mutation and symptomatic status, Bateman said. One site alone noted a database of 50 families with early onset AD that looked autosomal-dominant in their inheritance pattern, but lacked genetic verification. “We will follow up on these leads,” Bateman said. DIAN is already expanding in other ways. This year, the network is adding the Mayo Clinic, Jacksonville, Florida, as the eighth participating U.S. site, as well as two sites in Germany, Morris noted.
To engage physicians and individuals from around the world, the network has launched an online portal called the DIAN Expanded Registry (see ARF related news story). Officially announced in April of this year, the portal has brought in some 65 registrants so far, Bateman said. He stressed that the DIAN Expanded Registry is targeting specifically the small autosomal-dominant slice of the AD population, not all people interested in prevention trials for AD. For Alzheimer’s prevention trial participation more generally, the Alzheimer's Prevention Initiative is launching a larger registry. For people who have a diagnosis, the Alzheimer's Association’s TrialMatch service is available online or over the phone (1-800-747-2979). These three registries target slightly different populations, and their representatives pledged to coordinate among each other by referring interested individuals who came through a respective group’s door to the registry that best matches their situation.
Wanted: The Best Test
At the same time that investigators reach out to find participants, they are also working internally to define the outcome measures that are most likely to pick up the subtle changes expected to occur in the years prior to dementia. A drug’s potential success at preventing a person’s transition from asymptomatic to symptomatic will require the cognitive measures to be significantly more sensitive than those used in trials of mild to moderate AD. The DIAN Pharma Consortium asked a working group to pressure-test whether cognitive tests in DIAN are up to the task. This work is ongoing, and longitudinal data are not available yet, but in D.C., Martha Storandt from WashU briefed the group on cross-sectional data gathered up to March 2012. These suggest that most of the 22 cognitive tests DIAN participants take indeed detect differences between asymptomatic and symptomatic mutation carriers. Likewise, presymptomatic carriers had lower scores on most tests than did non-carriers. On certain tests, older carriers performed worse than young carriers, whereas both young and older non-carriers performed well. On rare tests, all participants performed worse if they were old than if they were young, but carriers of all ages had lower scores than did non-carriers. One advantage of testing and detecting differences in this younger population is that age had a lesser effect on cognitive performance.
Jessica Langbaum of the Alzheimer’s Prevention Initiative at Banner Alzheimer’s Institute in Phoenix, Arizona, briefed the group on the API’s parallel effort to pin down a handful of tests that change the most over time during the presymptomatic period, yet vary the least from person to person (for details, see ARF related news story). The winning combination of tests was similar for a sporadic and for an autosomal-dominant cohort; both included recall of word lists and paragraphs. Interestingly, the top five were slightly different if the task was to detect decline in the 10 years prior to AD diagnosis than if it was to detect decline four years prior, Langbaum said. Working with Suzanne Hendrix at Pentara Corporation, the scientists have in recent weeks further tested these composites by comparing them against either individual tests or a large battery, or by switching out certain tests. Each time, the original handful yielded the most power. “We have used different analytical approaches to ensure these results are robust,” Hendrix said.
Reisa Sperling at Brigham and Women’s Hospital in Boston, and colleagues have taken a similar approach in other datasets as part of their work preparing for the Anti-Amyloid Treatment in Asymptomatic AD (A4) trial to be run by the Alzheimer's Disease Cooperative Study. This is a third initiative to get secondary prevention trials off the ground. These scientists, too, are finding word list and paragraph recall tests to be particularly powerful, Sperling told the assembled group in Washington. The scientists at this meeting intensely discussed this question, as numerous groups are currently trying to validate composite test batteries for those coming trials. The leaders of the DIAN, API, and A4 prevention trial initiatives have agreed to seek consensus on what the best composite might be, and to use at least overlapping measures in their respective trials such that results can be compared directly or even be analyzed together.
New DIAN Data
At this meeting, Bateman for the first time presented a glimpse of what kind of longitudinal data scientists can expect soon. By March 2012, some 40 DIAN participants have had two of each type of assessment (clinical, neuropsychological, MRI, FDG, PIB, CSF), and seven participants had three. By the end of this year, the number of baseline visits is projected to stand at 308; 100 people will have come for two visits, 60 people for three visits, and 10 will have completed their fourth. As the longitudinal data are coming in, they are being analyzed to estimate power for the planned trials.
Tammy Benzinger of WashU offered the latest cut of cross-sectional and some longitudinal PIB-PET imaging. Asymptomatic carriers show the first signs of amyloid deposition around 18 years prior to expected age at onset. From there, deposition spreads and becomes AD-like, even before the clinical dementia rating budges from 0 to 0.5. That spread appears to happen at roughly the same rate in each affected brain region, Benzinger said. Longitudinal data are beginning to show that, for each brain region, baseline and follow-up PIB measures correlate, such that uptake increases on the second compared to the first scan, Bateman added. How many participants a trial would need for PIB to detect a treatment effect depends on whether the treatment reduces the rate of amyloid growth, halts its growth, or even reduces the absolute amount of brain amyloid, as has been reported for two different immunotherapies (Rinne et al., 2010; Ostrowitzki et al., 2011). Thirty people per arm would be highly powered to see at least the last effect, Bateman said.
Furthermore, Bateman noted that the amyloid loads measured in DIAN, as well as other parameters such as standard deviation and annual increase in deposition, are comparable to those published for other MCI or AD observational cohorts such as ADNI and the Australian Imaging, Biomarkers & Lifestyle Flagship Study of Ageing (AIBL).
These data raise the question of which amyloid PET tracers to choose for AD prevention trials. To help the clinical and pharma scientists address it, Victor Villemagne of Melbourne University, Australia, compared published data on the three most developed of the available candidates, florbetapir/Amyvid, flutemetamol, and florbetaben. All three stick to white matter longer than PIB, their signal is weaker, and their dynamic range smaller. Among these three 18F compounds, there are small differences as well. Therefore, these three 18F tracers are unlikely to pick up the very beginnings of amyloid deposition as sensitively as does PIB, said Villemagne. However, each of them is well capable of detecting whether there is significant amyloid in a prospective study participant’s brain, Villemagne added. Each can predict progression and support subject selection for trials. The tracer’s response to drug remains unproven, though florbetapir is being used in some ongoing AD therapeutic trials.
Florbetapir gained FDA approval for clinical use and is supported by Eli Lilly and Company; hence, it is likely to be available in the long run for trials that will last multiple years. Florbetaben was sold to the Indian company Piramal Imaging; Phase 3 autopsy data were presented at the American Academy of Neurology Conference in April of 2012 in New Orleans, Louisiana. GE Healthcare’s flutemetamol just completed an autopsy study and a biopsy study (see ARF related news story). A fourth compound, 18F-AZD4694, appears promising in early studies, with a signal much like PIB’s, but has not reached Phase 3 yet.
Villemagne works with Chris Rowe in a nuclear medicine center that tests all experimental amyloid tracers it can obtain. Asked essentially which tracer was the fairest of them all, Villemagne’s dodge injected a moment of levity into otherwise serious proceedings, “That I leave up to you. We practice promiscuity.”
Bateman presented Anne Fagan’s latest fluid biomarker data, which, like PET imaging, are beginning to include longitudinal results as DIAN participants undergo their second lumbar punctures. As expected, plasma Aβ40 is the same in non-carriers as in both asymptomatic and symptomatic carriers. Plasma Aβ42 is higher in carriers, but the data overlap and no clear age effect jumps out. Plasma Aβ42 does not differ strongly whether carriers are 30 years or five years away from their expected age at onset, Bateman said. Fagan and Bateman also showed data comparing DIAN’s CSF data to published data in sporadic cohorts using ADNI cutoffs. This comparison is limited because ADNI cutoffs were established with the help of an autopsy series and cognitive assessments, whereas the DIAN data come from living and, in large part, cognitively normal subjects, and were measured in different labs. With these provisos, the general trend in both sporadic and familial AD is that the amount of CSF Aβ42 in symptomatic individuals is reduced to about half that in controls, whereas tau and phospho-tau rise two- to threefold. “The take-home message is that DIAN CSF data are similar to sporadic AD CSF data,” Bateman said.—Gabrielle Strobel.
DIAN: What Sayeth the Regulator? Q&A With Rusty Katz
When the Dominantly Inherited Alzheimer Network (DIAN) convened its Pharma Consortium on 14 April 2012 in Washington, D.C, its scientists intended to brief the Food and Drug Administration on how far DIAN’s work has advanced to date (see Part 1). Their other goal was to obtain feedback from the FDA on the study designs DIAN trialists have proposed. To this end, DIAN Pharma Consortium (PC) members asked the advice of Russell Katz, who directs the agency’s neurology products division. A paraphrased and abbreviated Q&A of the conversation follows.
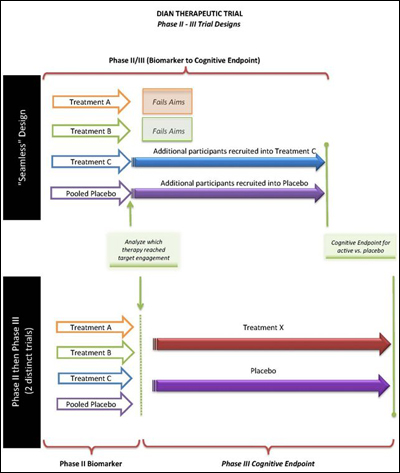
DIAN PC: Are there regulatory concerns in our choice of a so-called seamless design, where a biomarker phase runs into a longer Phase 3 trial, which then uses cognitive outcome measures?
Seamless trial design proposed by DIAN Therapeutic Trials Unit. View larger image. Image credit: DIAN Therapeutic Trials Unit
Russell Katz: I see no particular regulatory challenges to a seamless design. You need to address blinding questions and assure us that a type 1 error is not inflated in the envisioned design. It’s best to lay that out prospectively. That has been done before. One more point: Let’s assume arm A gets dropped and arm C continues; presumably, then, participants in arm A will be moved to C. That is not a problem.
DIAN PC: Is the intra-individual rate of change an acceptable endpoint if the parent DIAN study data are used as the run-in baseline data for the biomarker and cognitive endpoint trials?
Russell Katz: Conceptually, the agency has no objections to using intra-individual change. How exactly you are planning to analyze it will be important.
DIAN PC: For example, what if a person’s 20 percent per year decline in DIAN decreased to a 0 percent per year decline during the trial?
Russell Katz: You’d have to show it is statistically significant, but that is an impressive change.
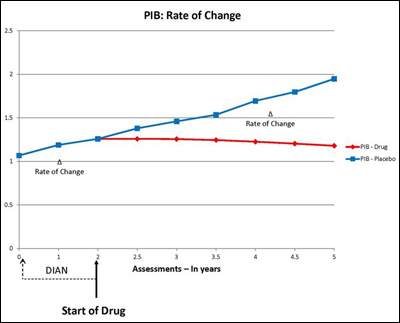
DIAN PC: Can DIAN use pre-trial data on biomarkers, CSF, imaging, clinical, and cognitive to determine a change, or individual rate of change? For example, can we use data that have been collected in DIAN as a baseline for evidence that a drug has changed PIB retention?
Hypothetical change in brain amyloid before and during treatment trial. View larger image. Image credit: DIAN Therapeutic Trials Unit
Russell Katz: Yes, this would be fine, assuming data collection was done post-randomization as it was done pre-randomization, i.e., during DIAN.
DIAN PC: Would the FDA concur, as indicated in November 2010 (see ARF related news story), that for individuals with autosomal-dominant AD and pre-manifest disease, a subtle clinical change in conjunction with an effect on a surrogate or even multiple surrogate markers could be acceptable for approval?
Russell Katz: Yes, we are open to that, for example, an effect on a composite cognitive measure.
DIAN PC: Would one such study be considered sufficient evidence?
Russell Katz: We are open to that, too. But the effect has to be robust, on the primary outcome, on the secondary outcomes. It has to be unassailable.
DIAN PC: If two drugs show benefit in the biomarker trial, are there any problems from a regulatory viewpoint of taking both forward (i.e., same placebo group, etc.)?
Russell Katz: I see no significant regulatory problem there.
DIAN PC: Would change in CDR-SOB as a single primary efficacy measure be suitable for registration?
Russell Katz: We are open to that. We have not signed off on that formally, but have told sponsors to flesh this out for us. We recognize that very early on, when people are asymptomatic, the usual rules are difficult to apply.
DIAN PC: Would a time-to-change outcome measure or a single cognitive measure or composite be sufficient for registration?
Russell Katz: Again, that is possible.
DIAN PC: How might these different endpoints affect the labeled indication if the trial is positive?
Russell Katz: It’s hard to know exactly what the label would say. We would be reluctant to grant a disease-modifying claim just on the basis of a clinical outcome. If you have a change on a biomarker and on a clinical outcome, then we contemplate granting a disease-modifying claim. What kind of a claim a positive trial would support also depends on whether all people who carry different mutations respond in the same direction.
DIAN PC: Based on FDA feedback to date, the agency prefers one IND holder, i.e., DIAN, with multiple product INDs, rather than the alternative of having multiple IND holders using the same protocol. What are the obstacles to having multiple IND holders?
Russell Katz: It is hard to imagine that we would accept multiple IND holders for the same trial. It would be a complicated trial and an administrative nightmare to deal with multiple sponsors. The regulations say that the sponsor is responsible for the conduct of the trial. There has to be one entity. With I-SPY, for example, that is the Foundation of the National Institute of Health (FNIH). I cannot imagine more than one IND holder.
DIAN PC: Under a single IND scenario, DIAN will need to meet certain obligations. DIAN will be responsible for IND amendments, safety reports, etc. Could these obligations, particularly those related to the reporting of serious adverse events (SAEs) to the FDA, be delegated or transferred to DIAN’s pharma partners?
Russell Katz: No. You can’t ask folks who are not the sponsor to handle an obligation of this sort that you are proposing. Amendments, safety, etc., have to come to us through the sponsor. Suppose there is a safety issue. It has to come to us; it has to be disseminated to all. How is that possible with multiple IND holders? I have asked about this idea internally, but we think it is not workable. I know it is of concern to some pharma partners. We are happy to sit down with the group to try to figure this out, but we are fairly clear the answer is no.
Russell Katz: What is the objection to a single IND holder?
DIAN PC member, speaking for the member's respective company, not the entire committee: It is not scientific or medical. Some companies are concerned about risk to their drug if they are not controlling the interaction with the FDA, especially if it is a drug that is under FDA review for approval based on other trials the company is also doing. For example, DIAN has not done much SAE reporting in a registration clinical trial. When an SAE comes in, sometimes it is difficult to determine if it is related to treatment, especially in such an unusual cohort.
Russell Katz: I don’t understand why it can’t happen under one IND holder. I have not heard anything today that would require multiple INDs, and see problems on our side coordinating separate studies with separate INDs.—Gabrielle Strobel.
NIH Director Announces $100M Prevention Trial of Genentech Antibody
Updated 21 May 2012
On May 21, the New York Times editorial page commented on this upcoming trial.
On 15 May at the Alzheimer’s Disease Research Summit 2012, a conference hosted by the National Institute on Aging, Francis Collins announced that $16 million of federal funds would go toward the first-ever therapeutic prevention trial in cognitively healthy people. The decision is part of the National Plan to Address Alzheimer’s Disease, said Collins, who directs the National Institutes of Health in Bethesda, Maryland. The unprecedented trial will be run by an international collaboration of researchers in academia and industry. The news came as Kathleen Sebelius, Secretary of the Department of Health and Human Services, formally introduced the long-awaited plan (see ARF related news story). Funding from a public-private partnership gives the green light to what is widely considered the cutting edge in the field of AD clinical research today, that is, the drive to evaluate mechanism-based experimental treatments in people who are on the path to Alzheimer’s but have not developed the disease’s neurodegeneration or symptoms yet.
The Alzheimer's Prevention Initiative is led by Eric Reiman, Pierre Tariot, and Jessica Langbaum at the Banner Alzheimer’s Institute in Phoenix, Arizona, and Francisco Lopera and his colleagues at the University of Antioquia in Colombia. Over the past two years, these scientists and other colleagues have enrolled members of the world’s largest kindred afflicted with a deterministic presenilin 1 mutation into a broad-based observational biomarker and cognition study while simultaneously laying the groundwork for secondary prevention trials. They consulted leading academic, biotech, and pharma researchers, regulators, and funders on the best approach. They navigated the legal and ethical challenges inherent in giving unapproved drugs to outwardly healthy people. The researchers got to know, and wrestled with finding, the most respectful ways of working with a vulnerable population living primarily outside of the U.S. (For background on API, see ARF related news story; ARF news story.)
Last fall, the scientists submitted to the National Institute on Aging a grant proposal for a first presymptomatic treatment trial in this population, as well as in people with autosomal-dominant AD mutations living in the U.S. The grant is being funded through $50 million from the 2012 NIH budget. In February, Sebelius had pledged that this money would be directed to select research projects this year (see ARF related news story). Slicing money out of the current fiscal year budget “is rarely done but was merited, given the urgency of this disease,” Collins said.
Scientists following the API’s progress have been curious about which investigational treatment the API scientists would choose as the most promising one to start with. Likewise, they wondered which pharma company would commit to making their leading experimental medicine available for a five-year trial in a genetically defined population while developing the drug for the much larger market of late-onset AD. The match eventually came to pass with Genentech of South San Francisco, a member of the Roche group.
A press release issued jointly by the Banner Alzheimer’s Institute and Genentech quotes its executive VP for Research, Richard Scheller, as saying: “Genentech is very excited to be a part of this landmark effort. If the study demonstrates that we can prevent the disease in this special group of patients, it may pave the way to preventing Alzheimer’s in the general population.”
Genentech licensed crenezumab from the Swiss biotech company AC Immune SA. Similar to bapineuzumab, solanezumab, and gantenerumab, three AD immunotherapies currently in Phase 3 and 2 trials, respectively, crenezumab is a humanized monoclonal antibody that binds the Aβ peptide. It differs in its technical details, such as which species of Aβ it binds and how strongly it activates microglial cells (see Alzforum Q&A with Ryan Watts). Watts is the lead scientist at Genentech on this project.
“The dominant mutations are definitely a model worth pursuing, as you can identify patients early,” said Rusty Katz, who directs the Food and Drug Administration’s Division of Neurology Products. Katz has advised the general process preparing for API trials over the years. Regulatory approval of this particular trial by the FDA and the Colombian drug regulatory agency Invima will take some months, putting the estimated start date for the trial into the first half of 2013, said Reiman.
Besides the NIH bolus, the $100 million trial gets $15 million of philanthropic funding coming through the Banner Alzheimer’s Institute, and Genentech will put up the rest. The company will also provide clinical and operational expertise to finalize design and conduct the study. Already, API scientists Langbaum, Yui Ayutyanont, and Suzanne Hendrix are collaborating with Carole Ho and others at Genentech to define a composite cognitive outcome measure and run power calculations.
Importantly, the trial is intended not as an exploratory study, but as a registration trial, meaning a positive outcome might form the basis for a new drug application, said Reiman. Toward this end, primary outcome measures will be a composite cognitive battery and other cognitive tools. Various brain imaging tests, including amyloid PET and fluid biomarkers, will be secondary outcomes.
Three hundred people in Colombia will participate in the trial. One hundred mutation carriers will receive monthly injections of crenezumab, 100 will get placebo, plus 100 non-carriers will receive placebo to ensure that study participants will not know whether they carry the pathogenic mutation or not. All participants will be asymptomatic, said Reiman.
In addition, some 24 people living in the U.S. will join the trial at five U.S. sites, said Reiman. The Banner Alzheimer’s Institute will be one; the others will be determined with the help of the Dominantly Inherited Alzheimer Network (DIAN), which collaborates with API. Genentech is a member of DIAN’s Pharma Consortium (see ARF related news story). Trial participants will be 30 years of age and older.
Conducting trials internationally can be a sensitive business, particularly in vulnerable genetic cohorts living in countries less affluent than the U.S. For his part, Lopera has been seeking a biopharma partner willing to recognize that. “We consider this a unique opportunity. These patients are a sacred group of people for Alzheimer’s research, and everything will be done with the utmost respect,” said Watts. “Genentech intends to provide study participants support for their time and efforts. We are currently working with Dr. Lopera and Banner on the details of this plan,” Ho wrote to Alzforum in an e-mail. API researchers themselves have set up a small nonprofit initiative to support the families' ongoing needs.
Should this trial work and the antibody eventually be approved, how will these families be able to afford a U.S.-made biologic therapy? “Genentech is committed to patients having access to our therapies. We have a number of patient access programs for our other therapies and will likewise ensure that the appropriate access to crenezumab is obtained after completion of the trial. We have discussed this with both Dr. Lopera and Banner,” Ho wrote to Alzforum.
Once the trial is complete, information will be made available to researchers worldwide. “We want to help develop faster ways for everybody to evaluate potential prevention drugs. It’s not just about testing this drug. It’s more broadly about helping the field link biomarker changes to clinical outcomes, and stimulating more prevention studies,” Reiman said. Ho confirmed that clinical data as well as placebo samples will be made available in an ADNI-like format after the trial is completed.
“In addition, Genentech and Banner intend to provide access to biomarker samples from treatment patients within 18 months of the completion of the five-year treatment period,” Ho wrote. This pledge is a highly unusual step. Companies generally refuse to share patient samples that contain their proprietary investigational drug. At this point, the prospect remains some seven years off into the future.
While this trial is gearing up, the API scientists are planning for the next one, which aims to test investigational drugs in ApoE carriers at elevated risk of developing Alzheimer’s. They also hope that this initial trial will stimulate more presymptomatic treatment trials throughout the field. They have developed an online registry as a tool to enable people to express their interest to join such trials in the future, and to help sponsors enroll the needed participants for such trials. Alzforum provides a quarterly newsletter in partnership with this registry.
The crenezumab trial was one of two announced as part of the National Plan to Address Alzheimer’s Disease. The other one is a five-year, $7.5 million trial headed by Suzanne Craft at the University of Washington, Seattle, to test whether an intranasal insulin spray improves cognition in 240 people diagnosed with mild cognitive impairment.
Secretary Sebelius came to present the historic plan on her birthday; she began her remarks after being serenaded by an auditorium full of conference attendees. Congressman Ed Markey (D) of Massachusetts was there as well. Markey cared for his mother when she had Alzheimer’s. He co-sponsored the National Alzheimer’s Project Act (NAPA), which mandates the implementation of a national plan. The plan is available for download.
However, aside from the trial news, the long-awaited unveiling of the plan felt a tad anticlimactic to scientists at the summit because it came without additional funds beyond those announced earlier this year. The scientific community is hoping for $1 billion to $2 billion to implement the plan’s stated goal of stopping Alzheimer’s by the year 2025. For now, speakers are limited to professing their resolve to making the plan more than a document. Ron Petersen, Mayo Clinic, Rochester, Minnesota, who chaired the NAPA advisory council, spoke about ways of monitoring progress and ensuring accountability. “Today marks a momentous occasion, but the work has just begun,” Petersen said. For her part, Sebelius concluded, “We look forward to the day when Alzheimer’s becomes another disease that hard work and partnership have beaten.”—Gabrielle Strobel.
This is Part 1 of a two-part series. See also Part 2.
Q&A With Ryan Watts, Genentech Lead Scientist on API Trial
Ryan Watts of Genentech is not only a researcher with a keen interest in the blood-brain barrier. He is also the founding research scientist on the clinical trial collaboration with the Alzheimer’s Prevention Initiative that NIH Director Francis Collins announced on May 15 at the 2012 NIA Research Summit in Bethesda, Maryland (see ARF related news story). Alzforum reporter Gabrielle Strobel spoke with Watts.
Q: In parallel to this upcoming prevention trial in autosomal-dominant Alzheimer’s disease that was announced yesterday, Genentech is developing crenezumab for late-onset AD. You are currently enrolling for a multicenter cognitive and a biomarker study in North America and Europe, both in Phase 2. In prior conversations, scientists at different pharma companies cited a perceived risk to their LOAD development program as a major reason for eschewing secondary prevention in a small population of mutation carriers (see ARF essay on prevention trials). How do you see this issue?
A: Therein lies the major reasoning behind crenezumab. We engineered this antibody to have reduced activation of microglia, the resident CNS immune cells. Our clinical studies thus far have shown no risk of vasogenic edema or microhemorrhage at doses in excess of other anti-Aβ antibodies. For us to move earlier in the progression of disease, the antibody needed to be safe. To go into a prevention trial where people do not have symptoms, it had to be very safe.
Recall that the origin of this field was active immunization marked by meningoencephalitis. Passive immunization has also been plagued by blood-brain barrier disruption seen as vasogenic edema and/or microhemorrhages. These observations have limited dosing and also raise concern about treating patients in a prevention setting. We have had the benefit of learning from these experiences. We engineered an anti-Aβ antibody that avoids these problems, and tested it in a large Phase 1 program that included ApoE4 carriers. We saw neither encephalitis nor vasogenic edema at relatively high doses, and thus feel motivated to do this prevention trial. We are enthusiastic about how important it is to go early and run a study like this. We also feel strongly about limiting patient risk.
Q: The other reason pharma was uninterested in the past is how long prevention trials in AD take. Five years!
A: If you have a defined genetic cohort and know when mutation carriers start to develop disease, then it becomes a different question. We are in it for the long run. We think this is a key clinical trial to test the amyloid hypothesis.
Q: Another argument I frequently heard is that trials in genetic mutations would not help get an indication for LOAD, the larger market.
A: Who knows what it means in terms of market size or labels? A purely commercial or purely regulatory perspective is not what drives us.
Q: Then what drives you?
A: Doing the right experiment. The concern is that researchers do their experiments in mild to moderate patients and, when those studies are negative, walk away, even though they never did the right experiment. Every biological pathway in AD will have an ideal time in the progression when that pathway is targetable. And there is no doubt that Aβ is a very early player.
We have an entire strategy for AD. We are going after several different molecular pathways besides Aβ. At this point in time, Aβ is a priority because of the genetic data, the clear runway, so to speak, of 10- to 15-year accumulation, and the availability of biomarkers. But as we go after cell death and neuroinflammation, for example, the concept that earlier is better does not automatically apply. Some pathways will likely be more active or targetable in later stages. Or consider the cholinesterase inhibitors or memantine, which are designed to enhance the function of the limited number of neurons that are still alive. It may not necessarily be better to take this type of drug in a preventive way.
Q: You have not thought about how the results of this API trial will affect registration for crenezumab?
A: It is too early to say if this type of study will allow us to make claims beyond this genetic cohort. Again, we run this study because it is the best scientific experiment to test the amyloid hypothesis in humans.
Q: How is crenezumab different from the other Aβ antibodies that are currently in Phase 2 and 3 trials?
A: We have a manuscript under review that describes its properties. Basically, crenezumab binds to oligomeric and fibrillar forms of Aβ with high affinity, and to monomeric Aβ with lower affinity. By comparison, solanezumab binds monomeric Aβ, and gantenerumab binds aggregated Aβ, as does bapineuzumab. Crenezumab binds all forms of the peptide.
Crenezumab is engineered on an IgG4 backbone, which allows it to activate microglia just enough to promote engulfment of Aβ, but not so strongly as to induce inflammatory signaling through the p38 pathway and release of cytokines such as tumor necrosis factor α. Crenezumab is the only IgG4 anti-Aβ antibody in clinical development that I am aware of. We have not seen vasogenic edema in our Phase 1 trials, which was the first main hurdle for us to overcome.
Q: Does that affect dose?
A: Yes. We can dose substantially higher than other anti-Aβ antibodies. For example, the bapineuzumab studies are dose-limited to 1 mg/kg as a result of vasogenic edema. Vasogenic edema resolved at 13 weeks. Hence, dosing for the Phase 3 was set at 1 mg/kg and 0.5 mg/kg once every three months in ApoE4 non-carriers, or 0.5 mg/kg in ApoE4 carriers. We are dosing as high as 15 mg/kg once a month. This generates a brain exposure that is between 10- to 100-fold higher. That is important.
By the way, one misconception along these lines warrants correction: Sometimes you read that solanezumab does not get into the brain, but bapineuzumab does. That is not true. Both get in at approximately a 1,000:1 ratio. In fact, most antibodies establish a steady-state ratio of approximately 1,000:1 blood-to-brain, unless they are uniquely engineered to cross the blood-brain barrier.
Bapineuzumab was the trailblazer to identify these risks. If you come into the field late, your goal is to engineer around these risks.
Q: The AD field is moving toward collaboration and data sharing. How about it?
A: This is part of the agreement with API. We are members of ADNI and understand the principle of data sharing. Data from this trial will be made publicly available.
Q: DIAN has a smaller number of asymptomatic carriers than does the API, and participants with dozens of different mutations in presenilin and APP, but is otherwise in a similar position. Are you interested in doing a similar thing with DIAN?
A: We are part of the DIAN consortium and believe all of these studies hold great promise.
This is Part 2 of a two-part series. See also Part 1.

{kind=link}
Comments
No Available Comments
Make a Comment
To make a comment you must login or register.