Potential Parkinson’s Treatments Target α-Synuclein, Cell Replacement
Quick Links
Current treatments for Parkinson’s patients help restore movement, but do not slow the underlying brain degeneration. Researchers are pursuing strategies to curb the accumulation of α-synuclein in hopes that this may delay disease progression. At the Society for Neuroscience annual meeting in Chicago October 17-21, scientists reported that two different drugs that promote α-synuclein clearance have completed Phase 1 safety testing, with biomarker results suggesting they are hitting their targets. Both are headed to Phase 2. Others reported on immunotherapy approaches in preclinical testing, including a strategy to disrupt α-synuclein deposits by targeting, of all things, tau oligomers. Meanwhile, after a decade-long hiatus, cell replacement strategies are gathering steam once again. Data on stem cell approaches, including one poised to enter Phase 1, intrigued the SfN crowd. Whether any of these treatments will pan out remains to be seen, but the talks reflected new momentum, with numerous disease-modifying therapies having entered the pipeline for Parkinson’s.
“I’m a huge fan of tackling α-synuclein. I think it’s the No. 1 target for Parkinson’s therapeutics,” said Jeffrey Kordower, Rush University, Chicago, who chaired a Parkinson’s symposium. Kordower noted that lowering α-synuclein might improve not only movement, but also non-motor symptoms, such as cognitive decline, for which no treatments currently exist. The non–motor symptoms typically lead family members to admit someone with Parkinson’s to a nursing home, he added.
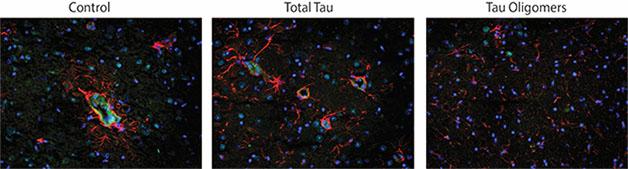
Target Tau to Treat PD? In untreated PD mice (left), and in those treated with an antibody to all forms of tau (middle), reactive astrocytes (red) swarm tau deposits (green). Mice treated with a tau oligomer-specific antibody (right) do not activate astrocytes. [Courtesy of Julia Gerson.]
In both Parkinson’s and dementia with Lewy bodies, deposits of aggregated α-synuclein accumulate in the brain. Because these aggregates, either as smaller oligomers or larger Lewy bodies, are believed to underlie disease symptoms, many groups are seeking ways to bust them up. At SfN, Fernando Pagan of Georgetown University, Washington, D.C., claimed the cancer drug nilotinib may do just that. Nilotinib, FDA-approved to treat adult chronic myeloid leukemia, inhibits the tyrosine kinase Abl. Abl phosphorylates α-synuclein and protects it from degradation via autophagy (see Mahul-Mellier et al., 2014). Inhibiting Abl seems to stimulate autophagic clearance of α-synuclein, Pagan said. His collaborator Charbel Moussa at Georgetown tested nilotinib in A53T mice, which overexpress mutant human α-synuclein and develop Lewy bodies. In these animals, 10 mg/kg of nilotinib given every other day for six weeks promoted autophagy of α-synuclein and of phosphorylated tau, lowering levels of these proteins by about half (see Hebron et al., 2013; Hebron et al., 2013; Hebron et al., 2015). Nilotinib treatment also pumped up brain dopamine levels and improved motor skills and cognition, Pagan reported at SfN.
Based on these data, Pagan and colleagues launched a Phase 1 study of the drug in 12 people with advanced PD or DLB at Georgetown University Hospital. For six months, participants received either 150 or 300 mg nilotinib daily, or about one-quarter the dose used for cancer treatment. At SfN, Pagan reported that participants tolerated the drug well, with no serious side effects. Since nilotinib can cause irregular heart rhythms, people with abnormal cardiac rhythms were excluded from the trial. At doses used in cancer treatment, nilotinib can also suppress the production of blood cells in the bone marrow. The participants maintained normal heart rhythms and blood cell production, Pagan reported.
The researchers tracked a suite of biomarkers. They found that plasma levels of α-synuclein dropped by more than half. CSF levels, which normally fall as Parkinson’s progresses, did not change. Tau and phosphorylated tau in CSF, which typically rise as cognition worsens, dropped. Other proposed CSF markers of neurodegeneration, such as S100B, also fell. Meanwhile, CSF dopamine levels climbed, causing the researchers to lower the dose of L-dopa given to some patients. Nilotinib appeared in CSF as well, indicating the drug entered the brain.
Participants self-reported that they functioned better on nilotinib, though that should be interpreted cautiously because there was no placebo control, the researchers said. Ten of the 11 participants who completed the trial reported meaningful improvements in their ability to speak, walk, and conduct daily activities, Pagan said. Those with DLB, or in earlier stages of PD, gained the most benefit. Improvements disappeared as soon as the drug was withdrawn, he added. The researchers plan to take the drug into Phase 2 in 2016.
Meanwhile, Curt Freed of the University of Colorado, Denver, presented a different approach to clearing α-synuclein. The Parkinson’s gene PARK7 encodes the protein DJ-1, whose many functions include protecting cells against oxidative stress and eliminating misfolded proteins. In primary neuronal cell cultures from A53T mice, DJ-1 blocks aggregation of mutant α-synuclein and prevents its toxicity (see, e.g., Zhou and Freed, 2005; Zondler et al., 2014). Looking for molecules that would increase DJ-1 expression, Freed and colleagues found that the histone deactetylase inhibitor phenylbutyrate roughly tripled DJ-1 levels. The FDA approved phenylbutyrate to treat rare metabolic disorders that prevent children from synthesizing urea. In mouse models of PD and DLB, the drug protected dopaminergic neurons and preserved motor and cognitive functions (see Zhou et al., 2011; Roy et al., 2012). Phenylbutyrate seemed to boost clearance of α-synuclein from the brain, since brain concentrations fell while plasma levels of the protein nearly doubled in treated mice, Freed noted.
Freed led a Phase 1 three-week biomarker study of the drug in 20 PD patients and 20 controls. Participants took 20 g per day, in the form of one teaspoonful of a liquid formulation with each meal. As in mice, treatment nearly doubled plasma α-synuclein, suggesting the drug promoted clearance from the brain. No safety issues cropped up, Freed said. This trial did not assess efficacy. The scientists are planning a Phase 2 trial to start in 2016, he wrote to Alzforum.
Phenylbutyrate has also been investigated for other neurodegenerative disorders, though it does not appear to be in any current trials for these indications. It was reported safe in a 2009 Phase 1 ALS trial (see Cudkowicz et al., 2009), and gave some hints of biomarker efficacy in a Phase 2 Huntington’s trial (see Oct 2011 news). In addition, phenylbutyrate treatment was reported to rescue cognition in Tg2576 AD mice (see Dec 2008 conference news). Freed noted that until recently, the drug was available only in pill form as sodium phenylbutyrate, so to reach the therapeutic dosage of 10 to 20 grams, participants would have to swallow 20 to 40 large pills each day. This may have curtailed interest in pursuing the therapy, he speculated.
Other research groups are trying to harness the immune system to sweep up α-synuclein aggregates. Antibodies against the protein restrict cell-to-cell transmission of α-synuclein in mice, suggesting immunotherapy might slow progression of PD (see Jun 2014 news). At least two anti-α-synuclein immunotherapies are in clinical trials, and more companies are developing such treatments (see Mar 2015 conference news and PRX002).
At SfN, Julia Gerson, who works in the lab of Rakez Kayed at the University of Texas Medical Branch, Galveston, described a different approach to Parkinson’s immunotherapy. Instead of targeting α-synuclein, she went after tau oligomers. Tau and α-synuclein oligomers occur together in Lewy bodies, and have been shown to cross-seed (see Apr 2003 news; Jul 2013 news; Lasagna-Reeves et al., 2010). The researchers previously generated a tau oligomer-specific antibody (TOMA) that crosses the blood-brain barrier and protects mouse models of tauopathy (see Castillo-Carranza et al., 2014; Castillo-Carranza et al., 2014).
Gerson injected a single dose of 120 μg of TOMA into the bloodstream of 17 seven-month-old A53T mice. This is the age when the mice start developing Lewy bodies and muscle weakness, which quickly progresses to paralysis. The authors waited two weeks, then tested behavior. The treatment preserved memory in the object recognition test as well as maintained gait. Treated mice built nests as ably as wild-types did, whereas untreated controls did not. In the brain, treated mice had fewer tau oligomers, more dopamine and dopaminergic neurons, and more synaptic proteins than untreated A53Ts, Gerson reported. The benefits seemed specific to this antibody, because treatment with an antibody that recognizes all forms of tau exacerbated behavioral defects, while a control IgG had no benefits, she added (see image above). Gerson is aging treated mice for 12 months to examine the long-term effects of treatment on behavior and brain pathology. Eventually, she would like to test a combination immunotherapy against both tau and α-synuclein, she said.
While many of the Parkinson’s immunotherapies under investigation employ antibodies, Marika Doucet of the University of Oxford, U.K., chose to pursue an active immunization strategy. Working in Richard Wade-Martins’ group, Doucet expressed fragments of α-synuclein on the surface of a virus-like particle (VLP) derived from a bacteriophage. Presenting the antigens in this way stimulates the immune system to generate antibodies against them. She tested the immunogenicity of three different α-synuclein fragments, one each from the C-terminus, middle, and N-terminus of the protein. Every month for two to three months, Doucet subcutaneously injected 20 μg of each VLP construct into SNCA-OVX model mice. These animals express wild-type human α-synuclein (see Janezic et al., 2013).
The vaccines based on the middle and C-terminal portions of α-synuclein both stimulated production of antibodies that recognized Lewy bodies in postmortem tissue from PD brains, she reported. After two to four months, titers were high enough that the antibodies would, in theory, cross the blood-brain barrier, although the researchers did not directly measure antibody levels in brain. Mice appeared healthy, with normal spleen, blood count, and body weight. However, the researchers saw no change in brain levels of aggregated or oligomeric α-synuclein. Doucet believes the vaccination protocol might have been too short and is now testing a one-year protocol.
Instead of clearing α-synuclein, other researchers are focusing on replacing dopaminergic cells damaged by the disease. This approach is unlikely to slow progression or improve non-motor symptoms, but it can lower the need for L-dopa treatment. Cell replacement fell out of favor a decade ago due to the inconsistent results and side effects seen with fetal dopaminergic grafts, but it has been buoyed by recent reports that some of these grafts remained healthy and provided motor benefits for as long as 20 years (see Jan 2014 news; Jun 2014 news). Now, many groups are turning to stem cells as a more controllable source for transplanted cells.
At SfN, Rodolfo Gonzalez of International Stem Cell Corporation, Carlsbad, California, described an approach using stem cells derived from unfertilized human oocytes by way of parthogenesis (see Jan 2002 news). Led by Eugene Redmond and Ruslan Semechkin, Gonzalez stimulated oocytes to divide to the blastocyst stage, then extracted pluripotent stem cells. These cells have the advantage of possessing two identical copies of every gene, including the human leukocyte antigen (HLA) gene, making genetic matching with patients easier, Gonzalez noted. The researchers had previously developed a protocol to differentiate these pluripotent cells into neural stem cells (see Gonzalez et al., 2013). The FDA has approved these cells for clinical trials, Gonzalez said. In a previous proof-of-concept study in 16 rats and two monkeys whose dopaminergic neurons were killed with toxins, the neural stem cells successfully engrafted into brain and pumped out dopamine (see Gonzalez et al., 2015).
At SfN, Gonzalez presented new data from a yearlong study in 20 African green monkeys. The researchers first injected the neurotoxin MPTP intramuscularly for one month to deplete dopaminergic neurons, then injected either 10 million neural stem cells, 20 million, or vehicle control into the striatum. All the monkeys that received stem cells had more surviving dopamine neurons in the substantia nigra at the end of the study than the control animals did, Gonzalez reported. However, only the low-dose group had more dopaminergic axons, higher dopamine levels in the striatum, and improved motor skills compared to untreated animals. None of the monkeys developed dyskinesia. None developed tumors, a potential side effect of stem cell implantation. The company plans to start a Phase 1/2a clinical trial in late 2015 in Australia and the United States., Gonzalez said. The trial will enroll patients in the early stages of PD.
Clinical trials of these cells might be premature, Kordower told Alzforum. He believes more basic research should first determine what type of cells these NSCs become, how many of them survive, and what exactly they do in the brain. Gonzalez did not address these issues in his talk, and could not be reached for comment. Kordower also works on stem cell programs for Parkinson’s.
Some groups in the stem cell field are transplanting mesenchymal stem cells (MSCs) into the brain rather than embryonic or pluripotent ones. Adult mesenchymal stem cells come from bone marrow and other tissues, making autologous transplant possible, and can be coaxed to differentiate into many cell types. In Chicago, Ryan Welchko in Gary Dunbar’s lab at Central Michigan University, Mount Pleasant, described one such approach. By expressing three transcription factors—Ascl1, Lmx1a, and Nurr1—in MSCs, the researchers induced them to differentiate into cells that resemble dopaminergic neurons. The cells expressed tyrosine hydroxylase, a key enzyme for producing dopamine, as well as dopamine transporters, and pumped out dopamine in culture.
To test the cells, Welchko and colleagues injected the toxin 6-OHDA into the striatum of one brain hemisphere of rats to kill dopaminergic cells. These animals developed poor limb control and a shuffling, slow gait reminiscent of Parkinson’s patients. After eight weeks, the researchers injected the differentiated cells into the brain. Two months later, they saw improvements in movement. Treated rats used their forelimbs for balance as well as wild-types, Welchko said. Typically, animals lesioned in one brain hemisphere spin in circles after being given the dopamine agonist amphetamine because only one side of their brain responds to the drug, but the treated animals spun less, indicating some restored dopaminergic function on the lesioned side. Next, Welchko will examine the brains of these animals to find out if injected cells survived and integrated into the brain circuitry.
With all of these strategies, potential pitfalls lurk as well. Kordower pointed out that because α-synuclein regulates synaptic function, lowering it too far could harm cognition. For cell-based therapies, researchers need to figure out how to avoid the dyskinesias that plague dopamine replacement approaches. Though the research still has a long way to go, speakers agree that scope of current therapeutic strategies has energized the field and generated a renewed sense of optimism for treating the pathology underlying Parkinson’s.—Madolyn Bowman Rogers
References
News Citations
- Tracking Huntington’s: Could Histone Protein Hit The Mark?
- DC: Developing But Debatable—Deacetylase Inhibitors for CNS Disease?
- Synuclein Snatch: Antibodies Snag Protein En Route to Next Neuron
- Antibody Against α-Synuclein Looks Safe In Phase 1
- Tau and α-synuclein at the Nexus of Alzheimer's and Parkinson's
- An Extra Strain on the Brain—α-Synuclein Seeds Tau Aggregation
- Parkinson's: Update on Gene Therapy, Fetal Cell Transplants
- Fetal Dopamine Grafts for Parkinson’s Remain Healthy After a Decade
- Primate Stem Cells by Parthenogenesis
Research Models Citations
Therapeutics Citations
Paper Citations
- Mahul-Mellier AL, Fauvet B, Gysbers A, Dikiy I, Oueslati A, Georgeon S, Lamontanara AJ, Bisquertt A, Eliezer D, Masliah E, Halliday G, Hantschel O, Lashuel HA. c-Abl phosphorylates α-synuclein and regulates its degradation: implication for α-synuclein clearance and contribution to the pathogenesis of Parkinson's disease. Hum Mol Genet. 2014 Jun 1;23(11):2858-79. Epub 2014 Jan 9 PubMed.
- Hebron ML, Lonskaya I, Moussa CE. Tyrosine kinase inhibition facilitates autophagic SNCA/α-synuclein clearance. Autophagy. 2013 Aug;9(8):1249-50. Epub 2013 Jun 19 PubMed.
- Hebron ML, Lonskaya I, Moussa CE. Nilotinib reverses loss of dopamine neurons and improves motor behavior via autophagic degradation of α-synuclein in Parkinson's disease models. Hum Mol Genet. 2013 Aug 15;22(16):3315-28. Epub 2013 May 10 PubMed. Correction.
- Hebron ML, Lonskaya I, Olopade P, Selby ST, Pagan F, Moussa CE. Tyrosine Kinase Inhibition Regulates Early Systemic Immune Changes and Modulates the Neuroimmune Response in α-Synucleinopathy. J Clin Cell Immunol. 2014 Sep 30;5:259. PubMed.
- Zhou W, Freed CR. DJ-1 up-regulates glutathione synthesis during oxidative stress and inhibits A53T alpha-synuclein toxicity. J Biol Chem. 2005 Dec 30;280(52):43150-8. Epub 2005 Oct 14 PubMed.
- Zondler L, Miller-Fleming L, Repici M, Gonçalves S, Tenreiro S, Rosado-Ramos R, Betzer C, Straatman KR, Jensen PH, Giorgini F, Outeiro TF. DJ-1 interactions with α-synuclein attenuate aggregation and cellular toxicity in models of Parkinson's disease. Cell Death Dis. 2014 Jul 24;5:e1350. PubMed.
- Zhou W, Bercury K, Cummiskey J, Luong N, Lebin J, Freed CR. Phenylbutyrate up-regulates the DJ-1 protein and protects neurons in cell culture and in animal models of Parkinson disease. J Biol Chem. 2011 Apr 29;286(17):14941-51. Epub 2011 Mar 3 PubMed.
- Roy A, Ghosh A, Jana A, Liu X, Brahmachari S, Gendelman HE, Pahan K. Sodium phenylbutyrate controls neuroinflammatory and antioxidant activities and protects dopaminergic neurons in mouse models of Parkinson's disease. PLoS One. 2012;7(6):e38113. Epub 2012 Jun 18 PubMed.
- Cudkowicz ME, Andres PL, Macdonald SA, Bedlack RS, Choudry R, Brown RH, Zhang H, Schoenfeld DA, Shefner J, Matson S, Matson WR, Ferrante RJ, . Phase 2 study of sodium phenylbutyrate in ALS. Amyotroph Lateral Scler. 2009 Apr;10(2):99-106. PubMed.
- Lasagna-Reeves CA, Castillo-Carranza DL, Guerrero-Muoz MJ, Jackson GR, Kayed R. Preparation and characterization of neurotoxic tau oligomers. Biochemistry. 2010 Nov 30;49(47):10039-41. Epub 2010 Nov 8 PubMed.
- Castillo-Carranza DL, Sengupta U, Guerrero-Muñoz MJ, Lasagna-Reeves CA, Gerson JE, Singh G, Estes DM, Barrett AD, Dineley KT, Jackson GR, Kayed R. Passive immunization with Tau oligomer monoclonal antibody reverses tauopathy phenotypes without affecting hyperphosphorylated neurofibrillary tangles. J Neurosci. 2014 Mar 19;34(12):4260-72. PubMed.
- Castillo-Carranza DL, Gerson JE, Sengupta U, Guerrero-Muñoz MJ, Lasagna-Reeves CA, Kayed R. Specific targeting of tau oligomers in Htau mice prevents cognitive impairment and tau toxicity following injection with brain-derived tau oligomeric seeds. J Alzheimers Dis. 2014;40 Suppl 1:S97-S111. PubMed.
- Janezic S, Threlfell S, Dodson PD, Dowie MJ, Taylor TN, Potgieter D, Parkkinen L, Senior SL, Anwar S, Ryan B, Deltheil T, Kosillo P, Cioroch M, Wagner K, Ansorge O, Bannerman DM, Bolam JP, Magill PJ, Cragg SJ, Wade-Martins R. Deficits in dopaminergic transmission precede neuron loss and dysfunction in a new Parkinson model. Proc Natl Acad Sci U S A. 2013 Oct 15;110(42):E4016-25. Epub 2013 Sep 30 PubMed.
- Gonzalez R, Garitaonandia I, Abramihina T, Wambua GK, Ostrowska A, Brock M, Noskov A, Boscolo FS, Craw JS, Laurent LC, Snyder EY, Semechkin RA. Deriving dopaminergic neurons for clinical use. A practical approach. Sci Rep. 2013;3:1463. PubMed.
- Gonzalez R, Garitaonandia I, Crain A, Poustovoitov M, Abramihina T, Noskov A, Jiang C, Morey R, Laurent LC, Elsworth JD, Snyder EY, Redmond DE Jr, Semechkin R. Proof of concept studies exploring the safety and functional activity of human parthenogenetic-derived neural stem cells for the treatment of Parkinson's disease. Cell Transplant. 2015;24(4):681-90. Epub 2015 Mar 24 PubMed.
External Citations
Further Reading
News
- Deep Brain Stimulation: It’s All About the Rhythm
- Tried and True: Levodopa Still Best First-Line Parkinson’s Medication
- New Parkinson’s Treatments Given Green Light
- Coenzyme Q10 Strikes Out in Phase 3 for Parkinson’s
- Could Bexarotene Treat Parkinson’s Disease?
- Barcelona: Parkinson’s Treatments on the Horizon
- Barcelona: Straight Talk From a Regulator on Trials in Parkinson’s
- First Phase 2 Success for Gene Therapy in Parkinson’s
Annotate
To make an annotation you must Login or Register.
Comments
No Available Comments
Make a Comment
To make a comment you must login or register.