Cognition Bump from Better Lifestyle: Due to Healthy Heart, Sound Sleep?
Quick Links
Back in July, the U.S. POINTER study showed that a structured lifestyle makeover in older adults slightly improves scores on memory and thinking tests (Baker et al., 2025; Aug 2025 conference news). At this year’s Clinical Trials on Alzheimer’s Disease conference, held December 1–4 in San Diego, clues emerged as to why. Supporting studies that tracked sleep quality, cardiovascular health, and brain pathology over the two-year trial suggest that, at least for now, the structured program’s benefits lie in fewer breathing-related sleep disturbances and better blood-pressure regulation rather than any shifts in amyloid or tau.
- Ancillary studies for U.S. POINTER report first results.
- Structured lifestyle program outperforms DIY approach for improving blood pressure regulation and sleep apnea.
- Alas, no differences in amyloid or tau pathology.
For a quick recap: The U.S. POINTER trial recruited just over 2,000 older Americans who barely exercised, ate poorly, and had at least two additional dementia risk factors: being over 70; having a family history of memory impairment; high blood pressure, cholesterol, or blood sugar; being male; or belonging to a racial or ethnic minority group. Volunteers were split into two groups and assigned to healthy lifestyle programs. Both emphasized exercise, brain training, nutritious eating, and social engagement, but one was more structured, offering personalized coaching and goal setting.
At the outset, participants could opt into several smaller studies alongside the main trial. One, POINTER Imaging, led by Susan Landau at the University of California, Berkeley, drew in roughly half of the full POINTER cohort. These participants averaged 68–69 years of age, and around 30 percent carried at least one APOE4 allele. Typically, 60–70 percent of people in Alzheimer’s research or memory clinic cohorts are APOE4-positive, making this group more representative of a typical slice of older Americans with modifiable risk factors, rather than the populations seen in many AD clinical trials. In this add-on, scientists measured amyloid and tau with PET scans and used MRI to gauge the size of participants’ hippocampi.
The intervention having wrapped up, Landau reported at CTAD that from baseline to the end of the two-year period, amyloid and tau PET signals rose a bit and hippocampal volume declined a bit—as would be expected in older adults—yet none of these measures differed between the structured and self-guided groups.
“Why didn’t we see any changes in our imaging biomarkers?” Landau asked on behalf of the audience. She noted that amyloid, tau, and structural measures shift slowly in cognitively unimpaired adults, and that two years may be too brief to see effects. “It’s still possible we’ll see a slowing in the accumulation of Alzheimer’s pathology,” Landau told Alzforum. “This could show up in certain subgroups—for example, people who were most engaged in the intervention, though we don’t have those data yet—or it might only become apparent over a longer follow-up period.”
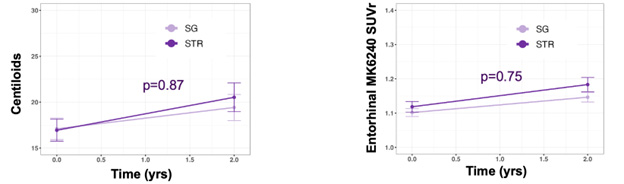
Pathology: Unperturbed. Despite healthier living, PET of amyloid plaques (left) and tau tangles in entorhinal cortex (right) show the expected age-related climb. [Courtesy of Landau et al., unpublished, 2025.]
Although no group differences emerged during the trial, participants’ baseline measures did appear to slightly influence how they responded to the intervention. Those who started out with smaller hippocampi seemed to experience slightly greater cognitive gains from the structured program than the self-guided one, whereas participants with larger hippocampi at baseline benefited equally from either intervention (image below).
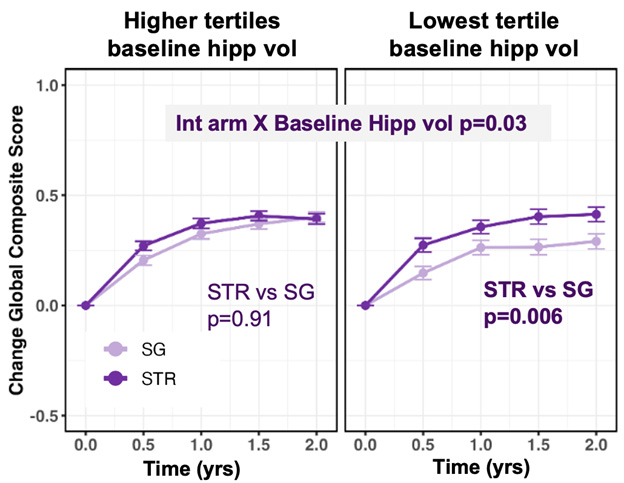
Brain Size Matters. Starting hippocampal volume shapes response. Participants in the top third of baseline hippocampal size (left) fared similarly across interventions, while those in the bottom third (right) did better with more structure. [Courtesy of Landau et al., unpublished, 2025.]
Perhaps surprisingly, baseline amyloid or tau had no bearing on which approach worked better. A similar pattern had been reported in the earlier JAMA publication: Participants who began with lower cognitive scores benefited most from the structured program, improving more than peers in the self-guided arm, while those who started with higher scores showed comparable gains across both interventions (Baker et al., 2025).
The CTAD audience also heard from Tina Brinkley of the Wake Forest School of Medicine, Winston Salem, North Carolina, who led POINTER-NV, the trial’s neurovascular arm. This study enrolled 491 participants—about one-quarter of the overall cohort. At baseline, 12 months, and 24 months, they underwent assessments such as transcranial Doppler and carotid ultrasound, a limited echocardiogram, and blood pressure and heart rate monitoring. Brinkley and colleagues found that in the structured arm, baroreflex sensitivity—a measure of the body’s ability to adjust blood pressure—rose by roughly 14 percent, a statistically significant gain. By contrast, this indicator rose only by a nonsignificant 3 percent in the self-guided group.
This finding matters, Brinkley emphasized, because regulating arterial blood pressure strongly influences cerebral blood flow, which has important consequences for cognitive function.
Laura Baker, POINTER’s lead investigator, also from Wake Forest University, presented findings from POINTER’s sleep study. It recruited 780 participants, 65 percent of whom had at least mild sleep apnea at baseline. At the start of the trial, and again at years 1 and 2, participants slept at home for a night wearing a WatchPAT home sleep apnea test. Researchers tallied apneas and hypopneas—drops in breathing lasting at least 10 seconds. By the study’s end, participants in the structured group had one to two fewer of these disturbances per hour of sleep compared with those in the self-guided group. This result may hint at why the structured group performed better on cognitive tests since poor sleep affects memory consolidation.
“We continue to be very pleased with the outcome of the U.S. POINTER trial for older Americans,” Baker told Alzforum. “We are fortunate to have an additional four years of observational follow-up, which will allow us to evaluate different time courses of intervention effects, as well as the durability of effects already reported.”
Further studies exploring the effects of healthier lifestyles were also presented in San Diego. Yen Ying Lim of Monash University in Melbourne, Australia, shared first data from the Better Brains trial, which tested whether an online, personalized lifestyle program could protect against cognitive decline in older Aussies with a first- or second-degree family history of dementia. “This is literally hot off the press—we finalized the data analysis last Thursday,” Lim told the audience.
Supported by a $3 million grant from the Australian Government’s National Health and Medical Research Council, recruitment began in 2019 but was cut short when COVID-related disruptions strained the team’s budget, Lim said, leaving enrollment a third below the original target. As such, more than 1,000 participants were randomized 1:1 into intervention and control arms. Their median age was 61; roughly four-fifths were women; three out of four lived in cities, the remainder in rural areas.
The trial was conducted entirely remotely. Half the participants got paired with a health-professional coach, who aimed to improve their eating habits, cardiovascular health, mood, sleep, and social engagement. The other half received educational materials but no structured guidance. The intervention lasted a year from randomization, followed by another year of observation, during which investigators checked in monthly to assess whether participants were meeting their goals.
At the two-year endpoint, slightly fewer participants in the intervention than the control arm showed cognitive decline on a battery of memory and thinking tests developed by the company Cogstate: 241 versus 256, a difference of about 7 percent. The p value of 0.0787 missed the conventional 0.05 threshold. Lim thinks that if recruitment had proceeded as planned, the trial likely would have been adequately powered to clear this hurdle.
CTAD attendees may have gone home thinking that healthy-living programs work wonders for keeping cognition sharp—that is, until Mark Espeland of Wake Forest University took to the stage. “It’s become apparent that multidomain lifestyle interventions have promise in slowing cognitive decline and perhaps even improving cognitive function, and that outcomes differ depending on whether the approach is intensive or less intensive,” he began. “What’s not apparent is whether these programs lead to long-term reductions in incident cognitive impairment—by which I mean MCI or dementia,” Espeland added.
Answering this question requires a large at-risk cohort with a follow-up period in the order of decades. The Look AHEAD trial, which Espeland helped lead, may offer this, at least in part (Look AHEAD Research Group et al., 2013).
The study set out to see how lifestyle changes might improve cardiovascular health in people with Type 2 diabetes. Starting in 2001, it signed up more than 5,000 people with diabetes—many of them overweight or obese—ages 45 to 76 from across the U.S. Participants were assigned either to an intensive lifestyle program focused on losing weight by cutting calories and getting more exercise, or to a control group that received educational materials. The intervention ran from 2004 to 2012, and researchers have been following up via phone interviews with participants ever since.
Both regimens helped participants lose some weight. As in POINTER, the intensive regimen had a slight edge: Participants lost an average of 13 pounds compared with 6 to 7 pounds in the control group at the end of the intervention. Even so, the scientists have seen no differences between groups in the rate of MCI or dementia after 15 years of follow-up.
Does this bode ill for POINTER? Perhaps not. Baker noted that Look AHEAD focused on Americans with Type 2 diabetes, the majority of whom were obese, a different population than POINTER, and also that its intervention protocols were different. “The FINGER study is probably a better predictor of whether we will see dementia risk reduction,” Baker told Alzforum.
That trial, the forerunner to POINTER, was led by Miia Kivipelto at the Karolinska Institute in Stockholm. In that study, all participants received basic health advice, and half joined an intensive program that paired structured dietary guidance with exercise classes and computerized cognitive training (Ngandu et al., 2015). Like POINTER, the structured arm showed small gains on cognitive tests relative to a self-directed cohort; further follow-up analyses are forthcoming.
Espeland, who was also involved in U.S. POINTER, echoed Baker’s point about the differences between the trials. Look AHEAD encouraged participants to walk, whereas POINTER asked for more intensive aerobic exercise. The diet prescriptions differed, and the diabetes cohort did not engage in cognitive training or increase their social activity. He noted that Look AHEAD’s cognitive data were collected after more than a decade of follow-up, and that the longer-term effects of U.S. POINTER remain unknown.—George R. Heaton
George Heaton is a freelance writer in Durham, North Carolina.
References
News Citations
Paper Citations
- Baker LD, Espeland MA, Whitmer RA, Snyder HM, Leng X, Lovato L, Papp KV, Yu M, Kivipelto M, Alexander AS, Antkowiak S, Cleveland M, Day C, Elbein R, Tomaszewski Farias S, Felton D, Garcia KR, Gitelman DR, Graef S, Howard M, Katula J, Lambert K, Matongo O, McDonald AM, Pavlik V, Raman R, Salloway S, Tangney C, Ventrelle J, Wilmoth S, Willliams BJ, Wing R, Woolard N, Carrillo MC. Structured vs Self-Guided Multidomain Lifestyle Interventions for Global Cognitive Function: The US POINTER Randomized Clinical Trial. JAMA. 2025 Aug 26;334(8):681-691. PubMed.
- Look AHEAD Research Group, Wing RR, Bolin P, Brancati FL, Bray GA, Clark JM, Coday M, Crow RS, Curtis JM, Egan CM, Espeland MA, Evans M, Foreyt JP, Ghazarian S, Gregg EW, Harrison B, Hazuda HP, Hill JO, Horton ES, Hubbard VS, Jakicic JM, Jeffery RW, Johnson KC, Kahn SE, Kitabchi AE, Knowler WC, Lewis CE, Maschak-Carey BJ, Montez MG, Murillo A, Nathan DM, Patricio J, Peters A, Pi-Sunyer X, Pownall H, Reboussin D, Regensteiner JG, Rickman AD, Ryan DH, Safford M, Wadden TA, Wagenknecht LE, West DS, Williamson DF, Yanovski SZ. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med. 2013 Jul 11;369(2):145-54. Epub 2013 Jun 24 PubMed.
- Ngandu T, Lehtisalo J, Solomon A, Levälahti E, Ahtiluoto S, Antikainen R, Bäckman L, Hänninen T, Jula A, Laatikainen T, Lindström J, Mangialasche F, Paajanen T, Pajala S, Peltonen M, Rauramaa R, Stigsdotter-Neely A, Strandberg T, Tuomilehto J, Soininen H, Kivipelto M. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial. Lancet. 2015 Jun 6;385(9984):2255-63. Epub 2015 Mar 12 PubMed.
Further Reading
No Available Further Reading
Primary Papers
- Baker LD, Espeland MA, Whitmer RA, Snyder HM, Leng X, Lovato L, Papp KV, Yu M, Kivipelto M, Alexander AS, Antkowiak S, Cleveland M, Day C, Elbein R, Tomaszewski Farias S, Felton D, Garcia KR, Gitelman DR, Graef S, Howard M, Katula J, Lambert K, Matongo O, McDonald AM, Pavlik V, Raman R, Salloway S, Tangney C, Ventrelle J, Wilmoth S, Willliams BJ, Wing R, Woolard N, Carrillo MC. Structured vs Self-Guided Multidomain Lifestyle Interventions for Global Cognitive Function: The US POINTER Randomized Clinical Trial. JAMA. 2025 Aug 26;334(8):681-691. PubMed.
Annotate
To make an annotation you must Login or Register.
Comments
No Available Comments
Make a Comment
To make a comment you must login or register.