In Early Trial, Vaccine Spurs Glut of Antibodies Against Aβ Aggregates
Quick Links
Monoclonal antibodies continue to show their ability to rid the brain of amyloid plaques. Trouble is, those antibodies need to be injected on the regular to keep taking down their targets in the brain. Active vaccines, on the other hand, turn the body into its own antibody factory. At the Clinical Trials on Alzheimer’s Disease conference, held December 1-4 in San Diego, Michael Agadjanyan of the Institute for Molecular Medicine, Huntington Beach, California, presented results from a small Phase 1 trial on AV-1959R, a vaccine against aggregated forms of Aβ. The immunization provoked robust and durable anti-Aβ responses in all 12 healthy participants who received it. While the jab triggered swelling at the injection site, it was otherwise well-tolerated and set off no serious complications. In a separate talk at CTAD, Lon Schneider of the University of Southern California, Los Angeles, laid out plans for a Phase 2 trial that will evaluate the vaccine in cognitively normal people with evidence of amyloid.
AV-1959R joins a handful of other Aβ vaccine contenders in Phase 1 and 2 trials. One is AC Immune’s ACI-24.060, which is being evaluated in a Phase 1b/2a trial in people with preclinical AD or Down’s Syndrome. Another is Vaxxinity’s UB-311, which demonstrated immunogenicity and a promising cognitive trend in a Phase 2 trial (Yu et al., 2023). Historically, therapeutic targeting of Aβ started with an active vaccine, AN-1792, ill-fated though it was, and some scientists in the field have privately bemoaned the discontinuation six years ago of Novartis' CAD106.
Of the currrent vaccines, ACI-24.060, UB-311 and AV-1959R all are equipped with some form of Aβ peptide, along with a cadre of non-self-antigens from common pathogens. These latter epitopes arouse both naïve and memory T-helper cells, which then inadvertently support B cells in their production of anti-Aβ antibodies. At CTAD, Agadjanyan claimed that not only did AV-1959R provoke higher antibody titers than either of these other two vaccines, but that it was also the only one to have done so in 100 percent of recipients.
AV-1959R uses the so-called Multi-TEP platform—a string of 12 Th cell epitopes that hail from tetanus toxoid, hepatitis B, and flu—to which three copies of the Aβ1-11 peptide are fused. The vaccine is prepared with the Advax-CpG adjuvant, a combination of polysaccharides and CpG oligonucleotides that further rouse the immune response. Nuravax, an Irvine-based biotech company of which Agadjanyan is president, is developing AV-1959R and other vaccines that use the Multi-TEP platform, including those directed against tau and β-synuclein. In San Diego, Agadjanyan showed results of a Phase 1, placebo-controlled trial, conducted in 16 healthy volunteers between 40 and 60 years of age. Two doses of AV-1959R—100 or 300 micrograms—were tested in two cohorts, each of which included six participants who received the vaccine and two who took placebo. Over the 22-week trial, participants received intramuscular injections of AV-1959R or placebo at baseline, week 4, and week 14, with the first two doses comprising the prime, and the third shot serving as the boost. Safety and tolerability were the primary outcomes, while secondary outcomes included measures of immunogenicity.
Both doses were deemed safe and well-tolerated, although they incited the discomforts typical of vaccines. Injection site reactions, characterized as pain, tenderness, or swelling, cropped up in 10 of the 12 participants in the vaccine groups, and two of four participants in the placebo groups. Six vaccinated and two placebo volunteers reported other generalized immunization reactions, such as chills, abdominal pain, vertigo, or headache. Of the 56 specific adverse events reported by participants across the entire trial, 49 were deemed mild and seven moderate in severity. None were serious.
Did AV-1959R spur antibodies against Aβ? Indeed it did. Agadjanyan reported that the vaccine was “extremely immunogenic.” In support of this, he first showed results of an ELISA, in which sera from participants was titrated onto plates containing Aβ42 protofibrils. At day 42—two weeks after receiving the second priming dose—all participants in the both vaccine dosing groups boasted high titers of Aβ-specific, IgG antibodies, while those in the placebo groups did not. Agadjanyan reported that at this timepoint, the concentration of anti-Aβ IgG antibodies in the blood topped 300 micrograms/mL, which is on par with steady-state levels reached by lecanemab and donanemab after injection of those monoclonal therapies. What’s more, B cells continue to produce these antibodies.
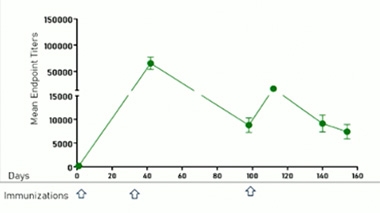
Persistent Prime. The concentration of anti-Aβ antibodies in the blood rose dramatically in response to priming with AV-1959R, with a smaller bump in response to the boost. [Courtesy of Michael Agadjanyan, Institute for Molecular Medicine.]
Curiously, fewer anti-Aβ antibodies rallied in response to the booster shot given at day 98 (image below). Agadjanyan attributed this to the high titers of remaining anti-Aβ antibodies that were stoked by the prime. If these antibodies take out the vaccine before it can reach the lymph nodes, this would put a damper on the booster response, Agadjanyan proposed. In support of this idea, people with the lowest concentrations of anti-Ab antibodies just prior to the boost mounted the greatest fold-increases in response to the booster, Agadjanyan told Alzforum. Weaving their antibody data into a statistical model, the scientists estimate that annual boosters of AV-1959R would be needed to maintain an effective armory of anti-Aβ antibodies.
To home in on which species of Aβ the antibodies recognized, the scientists teamed up with Charles Glabe at the University of California, Irvine, to generate peptides across the spectrum of aggregation—from monomers to oligomers to protofibrils to fibrils. After confirming these structures with electron microscopy, they plated them on nitrocellulose membranes with pooled sera from immunized participants. The scientists found that the vaccine-elicited antibodies bound most strongly to fibrils and protofibrils, latched on so-so to oligomers, and showed little interest in monomers (image below).
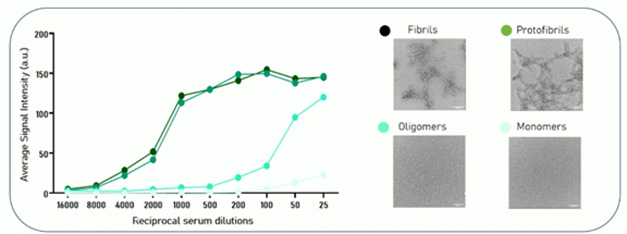
Attracted to Aggregates. Antibodies in pooled sera from AV-1959R-treated participants bound most tightly to fibrils and protofibrils, moderately to oligomers, and minimally to monomers (left). Aβ species visualized via electron microscopy (right). [Courtesy of Michael Agadjanyan, Institute for Molecular Medicine.]
In further support of their penchant for Aβ aggregates, antibodies from AV-1959R-immunized sera readily bound to Aβ plaques within brain sections from amyloidosis mice and from people with AD, Agadjanyan reported.
Whether the antibodies spurred by AV-1959R immunization engage their targets in the brain remains to be demonstrated. Agadjanyan showed no data on canonical AD biomarkers that might have addressed this question. However, the participants in this Phase 1 trial were healthy volunteers, not necessarily people with preclinical AD.
Cognitively unimpaired people with evidence of amyloid will be recruited for the planned Phase 2 trial. In San Diego, Schneider laid out the strategy for this secondary prevention trial. The trial will enroll at least 160 cognitively normal people with a plasma ratio of p-tau217/Aβ42 that indicates amyloidosis. Amyloid-PET will be used to exclude participants without plaques. Enrollees will receive 100 micrograms of AV-1959R or placebo at weeks 0, 4, and 44, and be tracked until the end of the study at week 78, when a second amyloid-PET scan will be performed.
Primary endpoints include safety and anti-Aβ immunogenicity, while secondary outcomes will assess changes to amyloid-PET as well as AD blood biomarkers. Cognitive and functional tests, as well as more detailed antibody and immune profiling, will be included among exploratory endpoints.
Agadjanyan and Schneider envision preclinical AD as the prime indication for AV-1959R. Agadjanyan believes that AV-1959R is a strong candidate for a Breakthrough Therapy designation, which, if granted, would speed up the FDA review process. Other Aβ vaccines, including ACI-24.060 and UB-311, have been awarded fast-track designation—a related status that also expedites FDA review. The Phase 2 trial is slated to start at the beginning of 2026.—Jessica Shugart
References
Therapeutics Citations
Paper Citations
- Yu HJ, Dickson SP, Wang PN, Chiu MJ, Huang CC, Chang CC, Liu H, Hendrix SB, Dodart JC, Verma A, Wang CY, Cummings J. Safety, tolerability, immunogenicity, and efficacy of UB-311 in participants with mild Alzheimer's disease: a randomised, double-blind, placebo-controlled, phase 2a study. EBioMedicine. 2023 Aug;94:104665. Epub 2023 Jun 29 PubMed.
Other Citations
External Citations
Further Reading
No Available Further Reading
Annotate
To make an annotation you must Login or Register.
Comments
Michigan State University
I have collaborated with Dr Agadjanyan in the past. I have injected mice with his Multitep vaccines and observed very high antibody titers. We published results with the tau vaccine (Joly-Amado et al., 2020). We also have unpublished data using the amyloid vaccine, confirming its efficacy in mice.
I do not have data comparing it to other recent vaccine approaches. However, it is more potent than the original Elan vaccine formulation we used 25 years ago (Morgan et al., 2000).
That said, I think for using vaccines as a therapeutic, rather than prophylactic, one needs to consider some issues that are less of a concern when using monoclonal antibodies.
The first consideration is that it is hard to unvaccinate someone. Some adverse reactions may require steroid treatments to resolve and do not spontaneously resolve as the antibodies are turned over, as with monoclonals.
Second, in the original AN1792 Elan vaccine trial, 6 percent of cases had significant adverse reactions which led to termination of the study at a very early stage. There is some evidence that these adverse reactions occured due to an aggressive T cell response to Aβ with T cell infiltration into the brain, although that has not been proven. It is anticipated that the Multitep vaccine would have less likelihood of an anti-Aβ T cell response because the major T cell antigens are not Aβ-related but are instead responding to viral and bacterial sequences in the Multitep sequences used to promote a strong immune response. Thus, it is the B-cell epitope in the N terminus of Aβ that should elicit the antibody reaction, but T cell responses should be against the non-self sequences in the vaccine peptide. Nonetheless, this is not a guarantee that no adverse T cell anti-self response will occur.
Third, the proposed clinical study plans to produce a rapid, large elevation of anti-Aβ antibody production, ultimately in people with existing Aβ deposits. This may elicit an ARIA reaction in these folks. Data on monoclonal antibodies suggest ARIA risk is reduced if the antibody dose is gradually titrated up, to avoid a rapid release of Aβ along the fluid transport pathways up the outside of the descending arterioles from the cortical surface. We and others have observed, in mice and humans, that many anti-Aβ immunotherapy approaches elevate vascular amyloidosis as it clears parenchymal deposits, and this is one factor that may contribute to ARIA. Thus, this rapid large elevation of anti-Aβ antibodies in the proposed study may increase the risk of ARIA. In the first participants who have amyloid deposits, the investigators might consider delaying the booster doses of the vaccine until the degree of ARIA risk with this approach is understood. Unless mouse studies are performed in aged mice, they are not always predictive of ARIA risk in humans.
Still, I believe that vaccines against amyloid will eventually greatly decrease incidence of or eliminate Alzheimer's dementia. I joked with Dr. Agadjanyan at the conference that they should add his vaccine to the one for shingles. The greatest success with vaccination is prevention, not therapy. I anticipate that around age 50 or so, amyloid-negative adults will be given anti-Aβ vaccines, which would lead to clearance of Aβ aggregates as they develop, and the centiloid threshold would never be breached. Then, Alzheimer's will become a memory.
References:
Joly-Amado A, Davtyan H, Serraneau K, Jules P, Zitnyar A, Pressman E, Zagorski K, Antonyan T, Hovakimyan A, Paek HJ, Gordon MN, Cribbs DH, Petrovsky N, Agadjanyan MG, Ghochikyan A, Morgan D. Active immunization with tau epitope in a mouse model of tauopathy induced strong antibody response together with improvement in short memory and pSer396-tau pathology. Neurobiol Dis. 2020 Feb;134:104636. Epub 2019 Oct 17 PubMed.
Morgan D, Diamond DM, Gottschall PE, Ugen KE, Dickey C, Hardy J, Duff K, Jantzen P, DiCarlo G, Wilcock D, Connor K, Hatcher J, Hope C, Gordon M, Arendash GW. A beta peptide vaccination prevents memory loss in an animal model of Alzheimer's disease. Nature. 2000 Dec 21-28;408(6815):982-5. PubMed.
Vice President, The Institute for Molecular Medicine
I want to clarify what I specifically claimed in my presentation (Slide 11) of CTAD-25: The adjuvanted AV-1959R vaccine induced a high level of anti-Aβ antibodies, with average endpoint titers above 1:65,000 after only two immunizations (priming), which is much higher than the levels of anti-Aβ antibodies reported in a subset of participants vaccinated seven times with ACI-24 (Rafii et al., 2022) and UB-311 (Wang et al., 2017; Yu et al., 2023).
Regarding Dr. Morgan’s comments, I would like to note that in monkey studies with the MultiTEP-based vaccines AV-1959 and AV-1980, we did not observe activation of T helper cells specific to Aβ and tau, respectively (Davtyan et al., 2014; Hovakimyan et al., 2022). I agree that the ARIA risk still exists with immunogenic vaccines, inducing high titers of anti-Aβ42 antibodies. However, the AV-1959R vaccine is intended for secondary preventive therapy in cognitively unimpaired individuals with evidence of amyloid pathology, with or without tau pathology. In these individuals, the target population for vaccination, there is significantly less Aβ42 in the brain than in individuals with early-stage AD. We envision that the AV-1959R vaccine might halt or at least slow the accumulation of pathological Aβ forms, with minimal risk of ARIA. Of course, only the large AV-1959R Phase 2 trial will allow us to further demonstrate the safety, immunogenicity, and efficacy of this vaccine in preclinical AD participants.
References:
Rafii MS, Sol O, Mobley WC, Delpretti S, Skotko BG, Burke AD, Sabbagh MN, Yuan SH, Rissman RA, Pulsifer M, Evans C, Evans AC, Beth G, Fournier N, Gray JA, Dos Santos AM, Hliva V, Vukicevic M, Kosco-Vilbois M, Streffer J, Pfeifer A, Feldman HH. Safety, Tolerability, and Immunogenicity of the ACI-24 Vaccine in Adults With Down Syndrome: A Phase 1b Randomized Clinical Trial. JAMA Neurol. 2022 Jun 1;79(6):565-574. PubMed.
Wang CY, Wang PN, Chiu MJ, Finstad CL, Lin F, Lynn S, Tai YH, De Fang X, Zhao K, Hung CH, Tseng Y, Peng WJ, Wang J, Yu CC, Kuo BS, Frohna PA. UB-311, a novel UBITh® amyloid β peptide vaccine for mild Alzheimer's disease. Alzheimers Dement (N Y). 2017 Jun;3(2):262-272. Epub 2017 Apr 14 PubMed.
Yu HJ, Dickson SP, Wang PN, Chiu MJ, Huang CC, Chang CC, Liu H, Hendrix SB, Dodart JC, Verma A, Wang CY, Cummings J. Safety, tolerability, immunogenicity, and efficacy of UB-311 in participants with mild Alzheimer's disease: a randomised, double-blind, placebo-controlled, phase 2a study. EBioMedicine. 2023 Aug;94:104665. Epub 2023 Jun 29 PubMed.
Davtyan H, Ghochikyan A, Petrushina I, Hovakimyan A, Davtyan A, Cribbs DH, Agadjanyan MG. The MultiTEP platform-based Alzheimer's disease epitope vaccine activates a broad repertoire of T helper cells in nonhuman primates. Alzheimers Dement. 2014 May;10(3):271-83. Epub 2014 Feb 20 PubMed.
Hovakimyan A, Zagorski K, Chailyan G, Antonyan T, Melikyan L, Petrushina I, Batt DG, King O, Ghazaryan M, Donthi A, Foose C, Petrovsky N, Cribbs DH, Agadjanyan MG, Ghochikyan A. Immunogenicity of MultiTEP platform technology-based Tau vaccine in non-human primates. NPJ Vaccines. 2022 Oct 12;7(1):117. PubMed.
Anavex Life Sciences
The Araclon A active immunotherapy, ABVac40, should also be mentioned in this context.
Vice President, The Institute for Molecular Medicine
Regarding Dr. Liedtke’s comment, I did not mention the AβVac4 vaccine because it does not target the N-terminal region of amyloid, which is the same region targeted by three FDA-approved monoclonal antibodies, Aduhelm, Leqembi, and Kisunla, as well as three other vaccines mentioned in this report. Instead, as reported by Alzforum, this vaccine consists of multiple small peptides from the C-terminus of Aβ40 spanning aa 33-40, fused to a KLH carrier.
Individuals aged 50-85 years with mild to moderate AD were immunized three times with ABvac40 formulated in Alum adjuvant. According to Lacosta et al., 88 percent of vaccinated individuals responded to the immunizations. Based on Table 3 of this published manuscript (Lacosta et al., 2018), nine participants had low antibody levels, with endpoint titers of 1:10, 1:30, 1:90 (n=2), 1:270 (n=2), and 1:810 (n=3). Five participants in this trial developed high antibody levels, with endpoint titers of 1:7290 (n=2), 1:21870 (n=2), and 1:65610 (n=2). Notably, in our validated ELISA, the average background antibody levels across all participants in the AV-1959R Phase 1 trials were 1:200.
References:
Lacosta AM, Pascual-Lucas M, Pesini P, Casabona D, Pérez-Grijalba V, Marcos-Campos I, Sarasa L, Canudas J, Badi H, Monleón I, San-José I, Munuera J, Rodríguez-Gómez O, Abdelnour C, Lafuente A, Buendía M, Boada M, Tárraga L, Ruiz A, Sarasa M. Safety, tolerability and immunogenicity of an active anti-Aβ40 vaccine (ABvac40) in patients with Alzheimer's disease: a randomised, double-blind, placebo-controlled, phase I trial. Alzheimers Res Ther. 2018 Jan 29;10(1):12. PubMed.
Make a Comment
To make a comment you must login or register.