Therapies Aim to Tame T Cells in the Brain
Quick Links
Cytotoxic T cells are star players in the adaptive immune system, enforcing protection against invading viruses or cancer cells. However, evidence has been mounting that the cells may also deal a neurodegenerative blow in people with AD and related diseases, where they invade the brain and wreak havoc (see Part 12 of this series). While scientists are catching on to a potentially destructive role of infiltrating cytotoxic CD8+ T cells in neurodegenerative diseases, therapeutic attempts to thwart their advances are popping up left and right. Some of those had results to show at this year’s AD/PD conference, held earlier this month in Vienna.
- Phase 1 and 2 trials of immunomodulatory drugs test ways to quell cytotoxic T cells beckoned to the AD brain.
- Low dose IL-2 and a nasal anti-CD3 antibody aim to expand T regulatory cells.
- In one approach, a person’s own rejuvenated natural killer cells purportedly get rid of troublemaking T cells.
One strategy is to bolster regulatory T cells. T-regs keep their killer cousins in check by secreting a portion of anti-inflammatory cytokines. Few T-regs reside in the brain, but a recent study did find a sparse yet potent population of them within the meninges. Removing them opened the floodgates for infiltrating CD8+ T cells (Feb 2025 news). Previously, scientists led by Alireza Faridar and Stanley Appel at Houston Methodist Hospital in Texas had shown that the suppressive power of T-regs was sapped in people with AD, but could be regained by expanding the cells in culture in the presence of the interleukin-2 cytokine (Faridar et al., 2020). When infused into immunodeficient 5xFAD mice, these human T-regs counteracted disease phenotypes (Faridar et al., 2022).
However, ex vivo expansion and reinfusion of T-regs is costly and laborious. Instead, this expansion can be spurred in vivo, by infusing low-dose IL-2. Because T-regs express a high-affinity receptor for IL-2, low doses of this cytokine spur their proliferation without fueling other types of T cells, which express lower-affinity receptors. Furthermore, scientists think that T-regs serve as an IL-2 sink, keeping the cytokine away from other T cells.
A small Phase 1 study that evaluated low dose IL-2 in eight people with AD cleared safety hurdles (Faridar et al., 2023).
In Vienna, Faridar presented findings from a Phase 2a proof-of-concept study of low dose IL-2, aka COYA 301, in 38 people with mild to moderate AD. Nineteen participants got placebo; 10 received IL-2 every two weeks, and nine every four weeks, for a total of 21 weeks. The primary endpoint was safety and tolerability, with T-reg numbers and CSF biomarkers/clinical measures as secondary and exploratory outcomes, respectively.
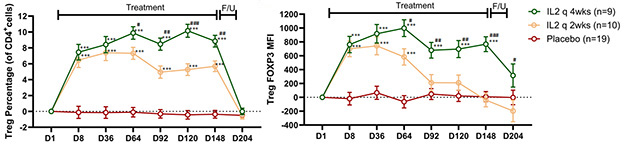
T-reg Bump. In participants who received low dose IL-2 every two weeks (yellow) or four weeks (green), but not placebo (red), both the T-reg percentage (left) and FoxP3 expression (right) increased relative to baseline. Monthly dosing maintained these effects for longer. T-regs returned to baseline during follow-up (F/U). [Courtesy of Alireza Faridar, Houston Methodist Hospital, 2025.]
All participants completed the six-month trial without serious adverse events. Treatment-related adverse events—elevated eosinophil count, redness at injection site, leukopenia—were mild and transient. T-regs rapidly expanded in the blood in response to both doses. Their numbers remained high in people receiving IL-2 every four weeks, but crept downward among those injected every two weeks (image above). Similarly, the expanded T-regs ramped up expression of the FoxP3 transcription factor, which mediates the suppressive function of the cells. FoxP3 remained elevated only in the monthly dosing group but dropped back down in the twice-monthly group. In Vienna, Faridar interpreted this as a sign of T-reg exhaustion due to an insufficient resting period between doses.
The scientists tracked a panel of 48 inflammatory mediators in plasma throughout the trial. Faridar reported that both IL-2 regimens lowered pro-inflammatory mediators CCL2, CCL1, and IL-15, while raising the anti-inflammatory cytokine IL-4. The monthly dose elicited the strongest changes in these markers. Faridar did not report effects on the other 44 plasma markers that were measured.
The treatment reportedly nudged some AD biomarkers in the right direction, raising CSF Ab42 while trending toward a stabilizing effect on CSF NfL and GFAP. It did not affect CSF p-tau181. Faridar noted trends on exploratory cognitive measures. People who received IL-2 every four weeks maintained stable scores on the ADAS-Cog and ADCS-CGIC, and declined 27 percent more slowly on the CDR-SB relative to the other two groups. Given the small, short trial, none of these differences were statistically significant. In toto, Faridar thinks the findings warrant a larger, longer trial of low-dose IL-2, and that the treatment might complement other disease-modifying drugs.
Howard Weiner of Brigham and Women’s Hospital in Boston has for many years been trying to nudge the neurodegenerative disease immune system in a therapeutic direction. In his family’s ancestral city of Vienna, Weiner presented results from a small trial testing a different way to bolster T-regs and quash cytotoxic T cells. Foralumab binds the TCR co-receptor, CD3. Weiner told Alzforum that how this antibody influences T cells varies depending on the immune environment into which it is introduced. When delivered intravenously, foralumab kills T cells, but when introduced into the mucosa, either orally or intranasally, it stimulates T-regs instead. For trials of AD and other disorders, the antibody is delivered as a nasal spray, a route which reportedly spurs the expansion and suppressive prowess of T-regs.
In the 3xTg mouse model of amyloidosis, nasal foralumab did not lower amyloid. It did, however, counter microglial activation, expand T-regs in the spleen and dCLNs, and promote the infiltration of CD4+ T cells into the brain, where they mingled with microglia (Lopes et al., 2023). Weiner told Alzforum that he believes these infiltrating CD4+ T cells are T-regs, although he did not check them for T-reg markers. The drug is currently in a Phase 2 trial in people with multiple sclerosis. Weiner said a pilot comparing 50 or 100 μg of foralumab to placebo in 16 people with mild AD is slated to begin within the month. Participants will take intranasal puffs three times per week for two weeks, followed by a one-week break, for six months.
In Vienna, Weiner also showed a glimpse of a response from one 78-year-old man with moderate-stage AD who received nasal foralumab as part of an expanded access program. The man underwent three-week cycles of nasal foralumab for three months, and received TSPO-PET scans before and after that period. Weiner reported a substantial drop in TSPO signal over the three-month period, suggesting that the treatment might be reducing microglial activation (image below). This one recipient is doing well and continues to receive foralumab treatments, Weiner reported.
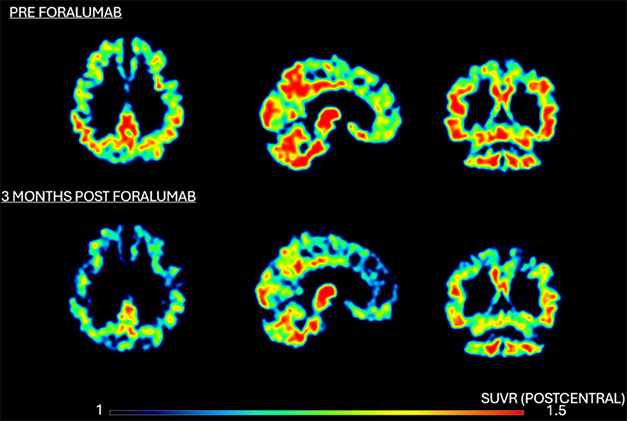
Calming Microglia? TSPO-PET scans at baseline and after three months of intranasal foralumab treatment suggest a drop in microglial activation. [Courtesy of Howard Weiner, BWH, 2025.]
Holtzman sees promise in this and other T-cell-targeted approaches. However, he thinks it’s important that their effects be relevant to the disease being targeted. For example, does the therapy at hand counter tau-mediated neurodegeneration?
For his part, Weiner sees potential for nasal foralumab in treating many neurodegenerative conditions where inflammation plays a hand. For example, he believes that foralumab might prevent the brain swelling that underlies amyloid-related imaging abnormalities (ARIA) in people receiving anti-Aβ immunotherapies. In support of this idea, a mouse study published last month, by Saef Izzy in Weiner’s lab and others, found that foralumab ameliorates brain damage and edema triggered by traumatic brain injury (Izzy et al., 2025). Weiner said that ongoing work led by Leah Beauchamp in his lab suggests foralumab counteracts harmful inflammatory responses in Parkinson’s models. Vikram Khurana at BWH will start studies in people with PD and MSA later this year, and an ALS study is in the works as well, Weiner said.
Kill the Killers
Another way of taking out cytotoxic T cells is to sic natural killer cells on them. Oncologist Paul Song of NKGen, a Santa Ana, California-based biotech, made this case in Vienna. Unlike T cells, which have one receptor to detect their target, NK cells are equipped with some 40 receptors with which they police the body for cells that need to be eliminated. “These can be cancer cells, virally infected cells, or renegade T cells that are attacking your own body,” Song said.
NK cells wane in number and potency with age. To correct this, scientists at NKGen have developed troculeucel. In this treatment, doctors collect a person’s NK cells via leukapheresis, the first step in CAR-T therapy. They expand them in culture in the presence of cytokines, a process that purportedly reawakens their killer instinct. They then freeze 30 to 50 aliquots of these invigorated executioners, which can be infused back into their original donor for months to come. NKGen has been evaluating this approach in ongoing cancer trials, and now, in AD. Song said that this move was motivated, in part, by improved cognition reported by cancer patients receiving the therapy.

Rejuvenate the Killers. Preparing the autologous NK cell treatment troceleucel involves collecting NK cells, expanding them in a cytokine stew, freezing aliquots, and returning them to the same person.
In Vienna, Song reported that during the ex vivo expansion phase, NK cells rev up expression of many of the receptors they use to sense prey. These include DNAM-1 and NKG2D, which detect autoreactive T cells. Song added that the cells also crank up CXCR3, a chemokine receptor that eases passage into the brain—and shows up frequently in microglia research. The souped-up cells phagocytosed aggregated Aβ42 and α-synuclein with great gusto, and killed activated, but not resting T cells, Song reported. These preclinical findings, along with results from a small, open-label dose-finding study conducted at a single center in Tijuana, Mexico, were recently published (Zúñiga et al., 2025).
This study tested four doses of autologous NK cells—ranging from 1 to 4 billion cells—in 11 people with mild to severe AD dementia. Participants received up to four infusions of their cells. It claimed to have found glimmers of a dose-dependent reduction in CSF GFAP, YKL-40, and p-tau181, which reportedly correlated with stabilization of cognitive scores on ADCOMS. It also reported that treatment-related adverse events, such as pain around the injection site and anemia, were mild.
Based on these early findings, NKGen asked the FDA about running a Phase 2a study in moderate AD, which would compare placebo to 17 doses of six billion NK cells. Because their initial dose-finding study didn’t have this high dose, the FDA requested NKGen first conduct a year-long Phase 1 study in people with moderate AD. In Vienna, Song showed results from this even smaller open-label study.
The three enrollees were women with moderate AD, who received 17 intravenous infusions of 6 billion of their own, rejuvenated NK cells every three weeks. Song said they suffered no treatment-related adverse events throughout the year-long regimen. He claimed that CDR-SB and ADCOMS scores improved over baseline in two of the women, and remained stable for the third. Plasma GFAP dropped and CSF Aβ42/40 rose for two of the three participants. Phospho-tau biomarkers remained stable throughout the trial, Song said.
A placebo-controlled Phase 2a trial in people with amyloid-PET confirmed moderate AD started enrolling earlier this year, and five people have enrolled so far, Song said. With the future goal of evaluating troceleucel in people with FTD, NKGen recently started the regimen in one person with FTD through a compassionate use authorization from the FDA (see press release). Mario Mendez and Jessica Rexach at the University of California, Los Angeles, are overseeing this study. The rest of the company’s products target various types of cancer.—Jessica Shugart
References
News Citations
Therapeutics Citations
Paper Citations
- Faridar A, Thome AD, Zhao W, Thonhoff JR, Beers DR, Pascual B, Masdeu JC, Appel SH. Restoring regulatory T-cell dysfunction in Alzheimer's disease through ex vivo expansion. Brain Commun. 2020;2(2):fcaa112. Epub 2020 Jul 20 PubMed.
- Faridar A, Vasquez M, Thome AD, Yin Z, Xuan H, Wang JH, Wen S, Li X, Thonhoff JR, Zhao W, Zhao H, Beers DR, Wong ST, Masdeu JC, Appel SH. Ex vivo expanded human regulatory T cells modify neuroinflammation in a preclinical model of Alzheimer's disease. Acta Neuropathol Commun. 2022 Sep 30;10(1):144. PubMed.
- Faridar A, Eid AM, Thome AD, Zhao W, Beers DR, Pascual MB, Nakawah MO, Roman GC, Davis CS, Grundman M, Masdeu JC, Appel SH. A phase 1 open-label pilot study of low-dose interleukine-2 immunotherapy in patients with Alzheimer's disease. Transl Neurodegener. 2023 Nov 16;12(1):54. PubMed.
- Lopes JR, Zhang X, Mayrink J, Tatematsu BK, Guo L, LeServe DS, Abou-El-Hassan H, Rong F, Dalton MJ, Oliveira MG, Lanser TB, Liu L, Butovsky O, Rezende RM, Weiner HL. Nasal administration of anti-CD3 monoclonal antibody ameliorates disease in a mouse model of Alzheimer's disease. Proc Natl Acad Sci U S A. 2023 Sep 12;120(37):e2309221120. Epub 2023 Sep 5 PubMed.
- Zúñiga CH, Acosta BI, Menchaca R, Amescua CA, Hong S, Hui L, Gil M, Rhee YH, Yoon S, Kim M, Chang PY, Kim YM, Song PY, Betito K. Treatment of Alzheimer's Disease subjects with expanded non-genetically modified autologous natural killer cells (SNK01): a phase I study. Alzheimers Res Ther. 2025 Feb 12;17(1):40. PubMed.
Other Citations
External Citations
Further Reading
Annotate
To make an annotation you must Login or Register.
Comments
No Available Comments
Make a Comment
To make a comment you must login or register.