Will We Soon Stage Alzheimer’s With Plasma Markers?
Quick Links
Cerebrospinal fluid and plasma markers are now being used to help diagnose Alzheimer’s in memory clinics, but what about using them to stage the disease? That’s the next big step, said Henrik Zetterberg, University of Gothenburg, Sweden, at this year’s ADPD meeting, held April 1–5 in Vienna. “At the last AD/PD, the theme was diagnosing amyloid positivity. This has gone well, and we can do that now. But we have to develop better tau markers for estimating tau load,” he said.
- Plasma eMTBR-243 tracks with tangles, especially at later stages of AD.
- P-tau217, with other plasma proteins, pegs people with lots of tangles.
- Combinations of p-tau markers may help identify stages of AD.
- This would help pick people best suited for therapy or clinical trials.
Scientists see several important uses for staging. For example, it can steer people more precisely to appropriate treatments. “With staging markers, we can screen out those with too much tau pathology who might be treated unnecessarily with anti-amyloid immunotherapy,” Zetterberg said.
Candidate staging markers are emerging. They run from eMTBR-243—a fragment of the microtubule-binding region of tau that can now be detected in plasma—to combinations of known phosphorylated and unphosphorylated tau isoforms, and to panels that include non-tau markers. Several groups of researchers are independently analyzing those approaches, competing to find the most accurate ones.
In Vienna, Kanta Horie, Washington University, St. Louis, presented new data on eMTBR-243. Unlike CSF MTBR-tau243, which can be detected by mass spectrometry after digesting samples with trypsin, the “e” version of MTBR detectable in plasma is formed by an endogenous proteolysis step, hence the “e.” At AAIC in Philadelphia last year, Randall Bateman from Wash U had explained how this marker picked out, with high accuracy, people who had tau pathology from among 165 volunteers in the Swedish BioFinder-2 and Knight ADRC cohorts (Aug 2024 conference news). Horie has expanded that to 739 people in the BioFinder-2 validation cohort, comparing eMTBR-tau243 with plasma p-tau217 and p-tau205. The work appeared in Nature Medicine online on March 31 (Horie et al., 2025).
Horie reported that eMTBR-tau243 is highly specific for tangles. While the percentages of phosphorylated tau 217 and 205 in plasma tick up in some cognitively impaired people who have no detectable tangles based on tau PET, eMTBR-243 is “zero” in those people, and even in people who do have low tangle levels, Horie said. Further, among people who are cognitively normal, eMTBR-243 levels were no higher in those who tested positive for amyloid than those who didn’t, suggesting plaques do not drive up this marker as they do for p-tau217 (image below).

Tangle Tracker? In BioFinder-2, plasma eMTBR-tau243 (green shaded areas, top) is more specific for Alzheimer’s disease than is plasma %p-tau217 (blue shaded areas, bottom). Gray dots indicate people who are tau-PET-negative, colored dots (green on top, blue on bottom) are tau-PET-positives, and white dots indicate PET data was not available. Dots are best seen by enlarging the image. For two R406W mutation carriers (pink dots), one with FTD had elevated eMTBR-tau243, while the other with MCI did not. Disorders with a “+” sign (x axis) are amyloid-positive. [Courtesy of Horie et al., Nature Medicine, 2025.]
Plasma eMTBR continues to climb the more tangles accumulate in a person’s brain, whereas p-tau217 and p-tau205 plateau (image below). This correlation between the marker and tangles is stronger in Braak stages III and above. According to multivariate modeling of these three markers, eMTBR-tau243 best captured tangles, whether people were amyloid-positive, tangle-positive, or both. “This marker may uniquely recapitulate mature tau tangle pathology, which p-tau species do not reflect,” concluded Horie. He believes eMTBR-tau243 could be used to stage AD tauopathy, or to determine if clinical symptoms are likely due to tangles.
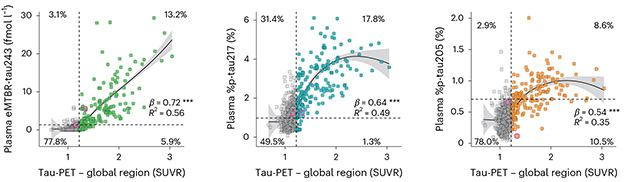
Early Versus Late. Plasma %p-tau217 (center) rises before global tau PET turns positive, then it plateaus. So does plasma %p-tau205 (right). Plasma eMTBR-tau243 (left) begins to rise later, after a positive PET scan, and continues to increase as more tangles accumulate. Gray dots indicate people who are tau PET-negative. Green (left), blue (center), and red (right) dots indicate people who are tau-PET-positive. [Courtesy of Horie et al., Nature Medicine, 2025.]
Oskar Hansson, Lund University, Sweden, and a co-author on the eMTBR-243 paper, echoed some of these points in his talk. “If you look in early Braak stages, then p-tau217 correlates with tau PET quite well, but at later stages eMTBR-tau243 is better,” he said. “It is a major predictor of tau pathology overall.” Hansson also reported that the MTBR fragment correlates more tightly than p-tau217 with brain atrophy and with cognitive decline, which are more sensitive to tangle burden than amyloid load. In short, Hansson thinks this marker could identify people with high tangle load.
Others in Vienna asked about the origin of eMTBR-243. One audience member wondered if it might be cleaved from tau by calpain 2, a protease that is more active in late AD. Horie said he does not know what enzymes are responsible but suspects lysosomal proteases or cathepsins.
That eMTBR-243 undergoes deamidation of asparagine 255 also piqued people’s curiosity. This natural post-translational modification is typically irreversible. Horie said that, in plasma, only the deamidated fragment correlates with tangles. He surmised this might be because non-deamidated tau from peripheral sources dilutes non-deamidated tau coming from the brain, skewing the data. In the CSF, on the other hand, both the normal and deamidated forms correlate with tangles equally well, he said. Where and how does this deamidation happen? That’s a mystery but, in their Nature Medicine paper, the authors speculated that the scene of the crime might be the tangles.
Make It a Panel
Zetterberg was intrigued by this possibility. He called the eMTBR-243 data a technical feat but noted that this marker is difficult to measure. It requires 1.2 mL of plasma and a mass spectrometer. “It is not implementable at large scale,” Zetterberg said. Plasma p-tau217 and other phospho-tau markers can more readily be measured by highly sensitive immunoassays; alas, they are not yet suitable for disease staging. What to do? Zetterberg thinks adding other markers to p-tau217 might be one way to go.
In Vienna, he showed preliminary results using the ultra-sensitive Nulisa immunoassay developed by Alamar Biosciences (Aug 2024 conference news). Using Alamar’s CNS panel of 126 markers, which include phospho-tau fragments and other peptides linked to neurodegeneration, Guglielmo di Molfetta, a Ph.D. student at the University of Gothenburg, asked which group of markers best distinguish people who have high and low tangle loads. Testing samples from 129 people in the Translational Biomarkers of Aging and Dementia cohort, aka TRIAD, at McGill University, Montreal, di Molfetta found that a foursome stood out: p-tau217, p-tau231, the astrocyte activation marker GFAP, and the neuronal pentraxin receptor NPTXR. The pentraxin NPTX2, together with 14-3-3γ, recently emerged as a marker of cognitive decline, both in aging and in people with familial or sporadic AD (Apr 2025 news). Tony Wyss-Coray, Stanford University, California, presented this data at AD/PD, and Zetterberg told Alzforum that the NPTX2/14-3-3γ-based synaptic health index Wyss-Coray devised could help clinicians decide whether an amyloid-positive person would benefit from treatment or might prefer to wait a few years.
Zetterberg showed that this foursome correlated better with high tangle load than did p-tau217, with AUCs of 0.94 and 0.88, respectively; age and sex were part of the equation. Using an alternative statistical regression method, called Lasso, di Molfetta turned up a slightly different panel, comprising p-tau217, NPTXR, glial-derived neurotrophic factor, and vascular growth factor. It performed similarly, with an AUC of 0.93.
The scientists tested this last panel on samples from BioFinder. Here, VGF contributed no predictive power, but p-tau217, NPTXR, and GDNF outperformed p-tau217 alone at spotting people with high tangle burden.
Next, di Molfetta repeated the Lasso regression on the BioFinder samples using Alamar’s full 126-marker CNS panel. Again, p-tau217, NPTXR, and GDNF popped up, along with fatty acid binding protein 3. FABP3 had emerged in the Triad analysis, too, though not as a top hit. Looking at just the common three markers, these still outdid p-tau217 alone, with AUCs of ~0.95 and ~0.93, respectively, at pegging people in late Braak stages in BioFinder.
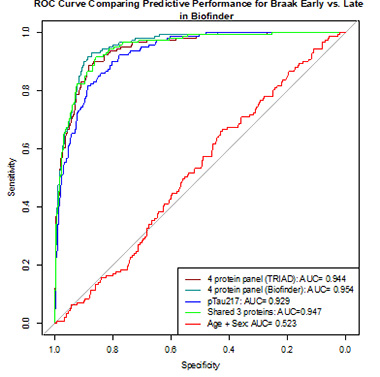
Panel's Best p-tau217. Top four hits from Triad (purple), top four from BioFinder (cyan), and the shared threesome (green) outperformed p-tau217 (dark blue) in picking out people with ample tangles. A model based on age and sex does about as well as flipping a coin (red). [Courtesy of Henrik Zetterberg, University of Gothenburg.]
“This is proof of principle that a panel can help improve tau staging,” Zetterberg told the audience. “The next step will be to compare with eMTBR-243, p-205, and NTA- [N-terminal tau fragments] tau, to see what happens if they are combined,” he said.
The Gothenburg team has investigated staging models based on most of these tau species. In the March 17 Acta Neuropathologica, scientists led by UGoth’s Andrea Benedet and Pedro Rosa-Neto, McGill University, reported that a pairing of p-tau217, p-tau205, and NTA-tau, in plasma or in cerebrospinal fluid, distinguishes people who have early, intermediate, and advanced tau pathology as per PET.
The work complements a CSF staging system reported last year by Hansson and Gemma Salvadó, also at Lund (Salvadó et al., 2024). It relied on Aβ42/40, p-tau217, p-tau205, tau’s non-phosphorylated mid region, and the CSF version of MTBR-tau243.
Benedet and colleagues used samples from TRIAD to establish their staging system. Co-first authors Juan Lantero-Rodriguez and Laia Montoliu-Gaya analyzed markers by immunoassay, except for plasma p-tau205. It was measured by mass spectrometry because there is no immunoassay for it in plasma. The scientists set cutoffs for each marker to establish four disease stages: 0—negative for all; 1—positive for p-tau217; 2—positive for p-tau217 and p-tau205; 3—positive for the two p-tau markers and for NTA-tau.
In a total sample of 219 people, 98 who were cognitively normal were amyloid-negative by PET; 89 percent of them were stage 0. Among 85 amyloid-positive people, those diagnosed with no cognitive impairment, mild cognitive impairment, or AD, had progressively higher stages (image below).
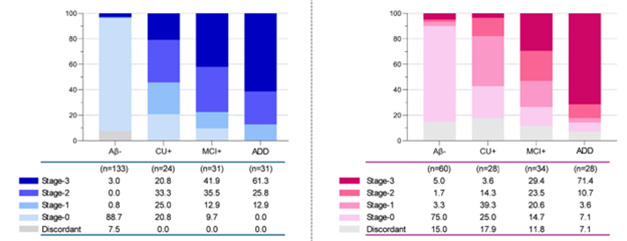
Dx by Stage. AD stage based on CSF (blue) and plasma (pink) levels of three tau markers aligned with clinical diagnosis. [Courtesy of Lantero-Rodriguez et al., Acta Neuropathologica, 2025.]
Among 150 people for whom plasma data was available, the distribution also shifted to higher stages with progressively worse diagnosis. That said, plasma-based staging lagged CSF-based staging, even in samples taken from the same person at the same time. This might indicate that it takes longer for these markers to make their way into the blood, the authors suspect. If that is true, then blood-based staging might underestimate how far someone is along the disease trajectory. “We would advise caution using plasma and CSF interchangeably to stage individuals,” Benedet told Alzforum.
This dichotomy comes from a small set of matched samples, which are hard to come by. “It is a matter of getting more data,” Montoliu-Gaya said, “If CSF and plasma [staging] truly don’t align, then we may need a different framework for plasma markers.” This is the first time scientists compared markers in matched plasma and CSF samples.
The TRIAD-based CSF and plasma staging schemes tracked well with groups defined by amyloid and tangle status, i.e., A-T-, A+T-, and A+T+, and by Braak stage (image below).
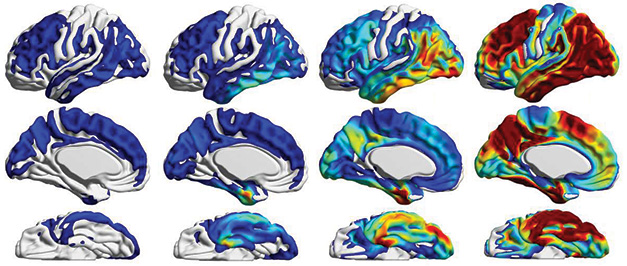
Plasma Versus PET. The four blood-marker-based stages (0 to 3 from left to right) correlated well with neurofibrillary tangle accumulation measured by tau PET. [Courtesy of Lantero-Rodriguez et al., Acta Neuropathologica, 2025.]
For their part, Salvadó and colleagues used mass spectrometry of CSF markers from 426 people in the BioFinder-2 cohort and modeled the most likely emergence of each along the disease trajectory with a machine learning algorithm dubbed Subtype and Stage Inference, aka SuStaIn (Oct 2018 news). This rendered six stages, 0 to 5, defined by sequential emergence of Aβ42/40, p-tau217/217, p-tau205/205, MTBR-tau243, and non-phosphorylated tau. As with Benedet et al.’s scheme, the number of people testing positive for amyloid and tau PET rose with each successive stage (image below).
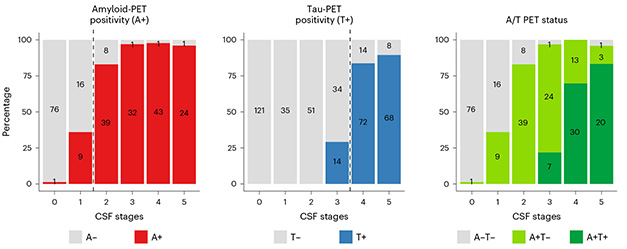
Stage Versus Path. SuStaIn algorithm created six stages of disease. The proportion of people positive for amyloid, tangles, or both, jumped with each successive stage. [Courtesy Salvadó et al., Nature Aging, 2024].
Salvadó tested this scheme on 222 CSF samples from the Knight Alzheimer Disease Research Center at Washington University. The staging sequence was the same, except for uncertainty about whether Aβ42/40 changed before p-tau217/tau217. For MTBR-tau243 and non-phosphorylated tau, the order was also unclear. Salvadó presented some of this data at the Human Amyloid Imaging conference, January 15-17 in San Juan, Puerto Rico (Feb 2025 conference news).
All told, the data suggest that the field is approaching a fluid marker staging system for AD that would offer a cheaper alternative to brain imaging in trials and, eventually, routine clinical settings. Both Benedet’s and Salvado’s systems placed p-tau205 after amyloid and before tangles. Last year’s revised criteria for diagnosis and staging of AD lumped p-tau205 in with T2 markers that signal presence of tangles, as opposed to T1 tau markers that reflect responses to amyloid (Jack et al., 2024). Benedet thinks p-tau205 could be a bellwether. “When deciding whether to treat people or exclude them from clinical trials, if p-tau205 is already going up, then it might be too late,” she told Alzforum.
Lantero-Rodriguez cautioned that the work to date is cross-sectional. “We need to see if this data holds up in longitudinal studies to learn if these markers and stages at baseline can predict future decline.”—Tom Fagan
References
News Citations
- A Plasma Test for Tangles?
- NULISA—A New Proteomic Method to Revamp Biomarker Analysis
- Do Synaptic Markers Foreshadow Cognitive Decline?
- Across Time and Space: Machine Learning Reveals Paths to Dementia
- At Human Amyloid Imaging Conference, Plasma Tau Was the Star
Paper Citations
- Horie K, Salvadó G, Koppisetti RK, Janelidze S, Barthélemy NR, He Y, Sato C, Gordon BA, Jiang H, Benzinger TL, Stomrud E, Holtzman DM, Mattsson-Carlgren N, Morris JC, Palmqvist S, Ossenkoppele R, Schindler SE, Hansson O, Bateman RJ. Plasma MTBR-tau243 biomarker identifies tau tangle pathology in Alzheimer's disease. Nat Med. 2025 Jun;31(6):2044-2053. Epub 2025 Mar 31 PubMed.
- Salvadó G, Horie K, Barthélemy NR, Vogel JW, Pichet Binette A, Chen CD, Aschenbrenner AJ, Gordon BA, Benzinger TL, Holtzman DM, Morris JC, Palmqvist S, Stomrud E, Janelidze S, Ossenkoppele R, Schindler SE, Bateman RJ, Hansson O. Disease staging of Alzheimer's disease using a CSF-based biomarker model. Nat Aging. 2024 May;4(5):694-708. Epub 2024 Mar 21 PubMed.
- Jack CR Jr, Andrews SJ, Beach TG, Buracchio T, Dunn B, Graf A, Hansson O, Ho C, Jagust W, McDade E, Molinuevo JL, Okonkwo OC, Pani L, Rafii MS, Scheltens P, Siemers E, Snyder HM, Sperling R, Teunissen CE, Carrillo MC. Revised criteria for the diagnosis and staging of Alzheimer's disease. Nat Med. 2024 Aug;30(8):2121-2124. PubMed.
Further Reading
Primary Papers
- Horie K, Salvadó G, Koppisetti RK, Janelidze S, Barthélemy NR, He Y, Sato C, Gordon BA, Jiang H, Benzinger TL, Stomrud E, Holtzman DM, Mattsson-Carlgren N, Morris JC, Palmqvist S, Ossenkoppele R, Schindler SE, Hansson O, Bateman RJ. Plasma MTBR-tau243 biomarker identifies tau tangle pathology in Alzheimer's disease. Nat Med. 2025 Jun;31(6):2044-2053. Epub 2025 Mar 31 PubMed.
- Lantero-Rodriguez J, Montoliu-Gaya L, Ashton NJ, Pola I, Therriault J, Rahmouni N, Brum WS, Servaes S, Stevenson J, Di Molfetta G, Arslan B, Klostranec J, Vitali P, Montembeault M, Gauthier S, Tissot C, Macedo AC, Pascoal TA, Jeromin A, Gobom J, Blennow K, Zetterberg H, Rosa-Neto P, Benedet AL. Biofluid-based staging of Alzheimer's disease. Acta Neuropathol. 2025 Mar 17;149(1):27. PubMed.
Annotate
To make an annotation you must Login or Register.
Comments
No Available Comments
Make a Comment
To make a comment you must login or register.