Confirmed: Lowering Blood Pressure Cuts Risk of Dementia
Quick Links
Because hypertension is linked to a greater risk of dementia, several trials have investigated whether lowering blood pressure in older people would protect the brain. Data from cohorts of a few thousand people point in that direction, but the findings have typically fallen short of statistical significance. In the April 21 Nature Medicine, scientists led by Jiang He at the University of Texas Southwestern Medical Center, Dallas, and Yingxian Sun at the First Hospital of China Medical University, Shenyang, presented some of the most convincing evidence yet for a protective effect. In a randomized trial of nearly 34,000 rural villagers with hypertension in China, those whose blood pressure was better managed had a 16 percent lower risk of all-cause dementia and mild cognitive impairment after four years than did those receiving standard care.
- In rural Chinese villages, intensive management of hypertension brought blood pressure below 130/80, while standard care did not.
- This low-cost intervention cut the risk of MCI and dementia by 16 percent over four years.
- If widely adopted, the approach could help lower the global dementia burden.
In a News & Views article, Josef Coresh at New York University Grossman School of Medicine, Salim Virani at Aga Khan University, Karachi, Pakistan, and Rebecca Gottesman at the National Institutes of Neurological Disorders and Stroke, Bethesda, Maryland, called the data compelling. “The study … provides critical evidence about the magnitude of dementia protection that can be realized by controlling blood pressure,” Coresh and colleagues wrote.
Smaller trials had consistently reported a trend toward fewer dementia cases in people who took antihypertensives compared with those who took placebo (Forette et al., 1998; Tzourio et al., 2003; Peters et al., 2008). Similarly, the larger SPRINT-MIND study of more than 9,000 people found a statistically significant 19 percent drop in new cases of MCI, and a trend toward less dementia, when blood pressure was managed aggressively rather than with standard care (Aug 2018 conference news; Jan 2019 news).
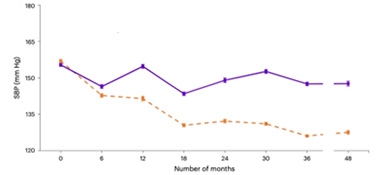
Lower Is Better. With intensive management (orange), the systolic blood pressure of Chinese villagers dropped by 22 mm Hg more over four years than with standard medical care (purple). [Courtesy of He et al., 2025, Nature Medicine.]
The China Rural Hypertension Control Project Phase-3 (CRHCP-3) afforded scientists the opportunity to address the issue in a larger population in a real-world primary care setting. In 326 villages, researchers tested blood pressure in all adults over 40 and recruited those with hypertension, defined as an untreated blood pressure ≥140/90 or a treated BP ≥130/80. The study enrolled 33,995 participants, or about 104 per village. They were 63 years old on average, and 61 percent were women. At baseline, their average BP was 156/88, they had been hypertensive for five to 10 years, and fewer than half were taking medication for it. Twenty percent had cardiovascular disease, nine percent had diabetes, and their cholesterol and blood sugar were fairly high.
In half of the villages, comprising 17,407 participants, scientists taught the local “village doctor,” who had some medical training but was not a physician, how to intensively manage blood pressure to bring it below 130/80. In the other villages, comprising 16,588 participants, the village doctors managed hypertension in the usual way. On average, people in the treatment group took three blood pressure medications; those in the control group, one. The treatment group complied more strongly, with 88 percent sticking to the regimen, versus 66 percent of the control group. In both groups, more than 90 percent of participants stayed in the trial until the end.
The intensive protocol was more effective than standard care, lowering blood pressure to 127/73, compared with 148/81 in the control group (image above). Looking at the data another way, two-thirds of the treatment group, but only 15 percent of the control group, ended up below the targeted BP threshold. The CRHCP study initially analyzed the effect of the intervention on cardiovascular disease, finding its incidence slashed by a third after three years (Sun et al., 2021; Sun et al., 2022; He et al., 2023).
To find out if the intervention staved off cognitive decline as well, joint first authors He and Chuansheng Zhao, Shanshan Zhong, Nanxiang Ouyang, Guozhe Sun, and Lixia Qiao, all at First Hospital of China Medical University, extended the study another year and added cognitive and functional outcomes. They administered the MMSE, the Functional Activities Questionnaire, and the Quick Dementia Rating System, and used the NIA-AA 2011 criteria for dementia (Apr 2011 news).

Overall, 5.4 percent of people in the control group developed dementia, versus 4.6 percent in the treatment group, for a risk ratio of 0.85. Results were similar for MCI, with its incidence falling from 21 to 17 percent, or a risk ratio of 0.84. The risk ratio for both outcomes combined was also 0.84, and was statistically significant at p <0.0001. The findings stayed unchanged after adjusting for potential confounders, including age, sex, education, smoking, and body mass index, as well as baseline cholesterol, blood sugar, and CVD.
Jurgen Claassen at Radboud University Medical Center, Nijmegen, the Netherlands, noted that CRHCP-3 extends findings from previous studies such as SPRINT-MIND by showing that the protective effect of lowering BP holds in a community setting, in a low- to middle-income country, and in ethnicities other than white people. In addition, the data imply that it is safe to aggressively lower BP, because there was no difference in falls or fainting between treatment groups, Claassen added (comment below).
Jason Hinman at the University of California, Los Angeles, picked up on the finding that blood pressure after treatment remained higher than in SPRINT-MIND, where doctors had tried to push systolic pressure below 120. This could indicate that absolute BP is less important than the amount of lowering. If so, interventions could be tailored to individual patients, he suggested (comment below).
CRHCP-3 participants started out with worse hypertension than in most other studies of BP and dementia, and the intervention resulted in a greater difference between groups. Nonetheless, the 15 percent risk reduction is in line with that in other studies. He and colleagues meta-analyzed their results with those from previous trials, and found a consistent 15 percent benefit. Previous meta-analyses have reported similar numbers (Hughes et al., 2020; Peters et al., 2022).
What is the protective mechanism? The CRHCP-3 made no attempt to differentiate between vascular dementia, Alzheimer’s disease, or other dementias, leaving this question unanswered. Scientists had previously estimated that 40 percent of all-cause dementia is vascular (Hachinski et al., 2019). “I would suspect that the lower all-cause dementia is related to both lower rates of cerebrovascular and Alzheimer’s disease, as cerebrovascular disease is a risk factor for AD,” Andrew Budson at Boston University wrote to Alzforum. Seth Love at the University of Bristol, U.K., noted that hypertension seems to contribute to dementia mainly by worsening arteriosclerosis, which weakens blood flow to the brain and disrupts the blood-brain barrier (Ruitenberg et al., 2001; Tayler et al., 2023).
Hypertension is the leading risk factor for death worldwide, with more than a billion people estimated to have it, less than half getting treatment, and only half of those reaching a healthy BP (Martin et al., 2024; World Health Organization 2023 report). The CRHCP-3 study demonstrates that it’s feasible to implement low-cost BP management in many countries, Coresh and colleagues said. The authors agree. “This proven-effective intervention should be widely adopted and scaled up to reduce the global burden of dementia,” He and colleagues suggested.—Madolyn Bowman Rogers
References
News Citations
- Could Better Blood Pressure Management Preserve Cognition?
- SPRINT MIND Data Published, Follow-Up Extended
- Revised Diagnostic Criteria for Alzheimer’s Are Published
Paper Citations
- Forette F, Seux ML, Staessen JA, Thijs L, Birkenhäger WH, Babarskiene MR, Babeanu S, Bossini A, Gil-Extremera B, Girerd X, Laks T, Lilov E, Moisseyev V, Tuomilehto J, Vanhanen H, Webster J, Yodfat Y, Fagard R. Prevention of dementia in randomised double-blind placebo-controlled Systolic Hypertension in Europe (Syst-Eur) trial. Lancet. 1998 Oct 24;352(9137):1347-51. PubMed.
- Tzourio C, Anderson C, Chapman N, Woodward M, Neal B, MacMahon S, Chalmers J, . Effects of blood pressure lowering with perindopril and indapamide therapy on dementia and cognitive decline in patients with cerebrovascular disease. Arch Intern Med. 2003 May 12;163(9):1069-75. PubMed.
- Peters R, Beckett N, Forette F, Tuomilehto J, Clarke R, Ritchie C, Waldman A, Walton I, Poulter R, Ma S, Comsa M, Burch L, Fletcher A, Bulpitt C, . Incident dementia and blood pressure lowering in the Hypertension in the Very Elderly Trial cognitive function assessment (HYVET-COG): a double-blind, placebo controlled trial. Lancet Neurol. 2008 Aug;7(8):683-9. PubMed.
- Sun Y, Li Z, Guo X, Zhou Y, Ouyang N, Xing L, Sun G, Mu J, Wang D, Zhao C, Wang J, Ye N, Zheng L, Chen S, Chang Y, Yang R, He J. Rationale and Design of a Cluster Randomized Trial of a Village Doctor-Led Intervention on Hypertension Control in China. Am J Hypertens. 2021 Aug 9;34(8):831-839. PubMed.
- Sun Y, Mu J, Wang DW, Ouyang N, Xing L, Guo X, Zhao C, Ren G, Ye N, Zhou Y, Wang J, Li Z, Sun G, Yang R, Chen CS, He J, CRHCP Study Group. A village doctor-led multifaceted intervention for blood pressure control in rural China: an open, cluster randomised trial. Lancet. 2022 May 21;399(10339):1964-1975. Epub 2022 Apr 29 PubMed.
- He J, Ouyang N, Guo X, Sun G, Li Z, Mu J, Wang DW, Qiao L, Xing L, Ren G, Zhao C, Yang R, Yuan Z, Wang C, Shi C, Liu S, Miao W, Li G, Chen CS, Sun Y, CRHCP Study Group. Effectiveness of a non-physician community health-care provider-led intensive blood pressure intervention versus usual care on cardiovascular disease (CRHCP): an open-label, blinded-endpoint, cluster-randomised trial. Lancet. 2023 Mar 18;401(10380):928-938. Epub 2023 Mar 2 PubMed.
- Hughes D, Judge C, Murphy R, Loughlin E, Costello M, Whiteley W, Bosch J, O'Donnell MJ, Canavan M. Association of Blood Pressure Lowering With Incident Dementia or Cognitive Impairment: A Systematic Review and Meta-analysis. JAMA. 2020 May 19;323(19):1934-1944. PubMed.
- Peters R, Xu Y, Fitzgerald O, Aung HL, Beckett N, Bulpitt C, Chalmers J, Forette F, Gong J, Harris K, Humburg P, Matthews FE, Staessen JA, Thijs L, Tzourio C, Warwick J, Woodward M, Anderson CS, Dementia rIsk REduCTion (DIRECT) collaboration. Blood pressure lowering and prevention of dementia: an individual patient data meta-analysis. Eur Heart J. 2022 Dec 21;43(48):4980-4990. PubMed.
- Hachinski V, Einhäupl K, Ganten D, Alladi S, Brayne C, Stephan BC, Sweeney MD, Zlokovic B, Iturria-Medina Y, Iadecola C, Nishimura N, Schaffer CB, Whitehead SN, Black SE, Østergaard L, Wardlaw J, Greenberg S, Friberg L, Norrving B, Rowe B, Joanette Y, Hacke W, Kuller L, Dichgans M, Endres M, Khachaturian ZS. Preventing dementia by preventing stroke: The Berlin Manifesto. Alzheimers Dement. 2019 Jul;15(7):961-984. PubMed.
- Ruitenberg A, Skoog I, Ott A, Aevarsson O, Witteman JC, Lernfelt B, van Harskamp F, Hofman A, Breteler MM. Blood pressure and risk of dementia: results from the Rotterdam study and the Gothenburg H-70 Study. Dement Geriatr Cogn Disord. 2001 Jan-Feb;12(1):33-9. PubMed.
- Tayler HM, MacLachlan R, Güzel Ö, Miners JS, Love S. Elevated late-life blood pressure may maintain brain oxygenation and slow amyloid-β accumulation at the expense of cerebral vascular damage. Brain Commun. 2023;5(2):fcad112. Epub 2023 Apr 4 PubMed.
- Martin SS, Aday AW, Almarzooq ZI, Anderson CA, Arora P, Avery CL, Baker-Smith CM, Barone Gibbs B, Beaton AZ, Boehme AK, Commodore-Mensah Y, Currie ME, Elkind MS, Evenson KR, Generoso G, Heard DG, Hiremath S, Johansen MC, Kalani R, Kazi DS, Ko D, Liu J, Magnani JW, Michos ED, Mussolino ME, Navaneethan SD, Parikh NI, Perman SM, Poudel R, Rezk-Hanna M, Roth GA, Shah NS, St-Onge MP, Thacker EL, Tsao CW, Urbut SM, Van Spall HG, Voeks JH, Wang NY, Wong ND, Wong SS, Yaffe K, Palaniappan LP, American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. 2024 Heart Disease and Stroke Statistics: A Report of US and Global Data From the American Heart Association. Circulation. 2024 Feb 20;149(8):e347-e913. Epub 2024 Jan 24 PubMed.
- Global report on hypertension: the race against a silent killer. World Health Organization.
Further Reading
No Available Further Reading
Annotate
To make an annotation you must Login or Register.
Comments
Radboud University Nijmegen Medical Center
This is a very relevant paper. It addresses several of the points raised in Elahi et al., 2023, which was written by ISAART members following a 2021 roundtable hosted by its Vascular Cognitive Disorders.
The SPRINT study indicated that intensive blood pressure control could be a strategy to prevent dementia, but in the perspective paper we wrote that SPRINT was done in a U.S. population, and we would need to see if effects translate to other ethnicities and in lower- to middle-income countries. This study does both, with its setting in rural China.
This study makes several important contributions. It uses a relatively cheap intervention (antihypertensive medication is very cheap and blood pressure devices are relatively cheap compared to other medical devices). And it appears that a complete village was treated by just one health care worker. This could be an example for other LMICs, but perhaps also for high-income countries that face health care challenges in the near future due to aging populations.
The study also addresses the safety concerns that always come up with intensive BP targets: Will it lead to orthostatic hypotension, falls, brain hypoperfusion? As we discussed in the perspectives paper cited above, recent research has shown that these safety concerns may be incorrect. For example, papers showing U-shaped BP curves which suggest that "going too low" may cause harm are often cited to say that intensive BP treatment targets could be unsafe. However, these U-shaped curves are likely an artefact caused by bias. The same applies to orthostatic hypotension: Recent studies suggest that intensive BP control does not necessarily increase the risk of orthostatic hypotension and syncope. This study supports the safety of setting an intensive BP target, because in the intervention villages there were no more adverse events than in the control villages.
The "village" design suggests that a more representative population was included than in "normal" RCTs such as SPRINT.
The absolute reduction of dementia by 1 percent from 5 percent in the control villages to 4 percent in the intervention, may not seem much, but it was achieved in just four years, and at low cost. And because the incidence of dementia increases with age, I estimate that the absolute reduction in dementia cases will increase further with longer follow-up.
References:
Elahi FM, Alladi S, Black SE, Claassen JA, DeCarli C, Hughes TM, Moonen J, Pajewski NM, Price BR, Satizabal C, Shaaban CE, Silva NC, Snyder HM, Sveikata L, Williamson JD, Wolters FJ, Hainsworth AH. Clinical trials in vascular cognitive impairment following SPRINT-MIND: An international perspective. Cell Rep Med. 2023 Jun 20;4(6):101089. PubMed.
Mary S. Easton Center for Alzheimer's Research and Care at UCLA
Large population-based studies, including ARIC, Framingham, and several large cohorts in Europe, have established a link between mid-life hypertension and the progression to mild cognitive impairment and dementia. Prior work from the SPRINT-MIND clinical trial demonstrated a trend, with strict lowering of blood pressure on the progression to mild cognitive impairment but not dementia. This study, while not a randomized controlled trial like SPRINT-MIND, does provide supportive evidence for aggressive BP lowering as a preventive strategy for dementia. The study adds to the wealth of data from the listed cohorts that blood pressure drives vascular changes in the brain that strongly associate with risk for dementia.
This study expands on the available data. Patients in this study had a higher mean starting SBP/DBP than those in SPRINT-MIND and did not achieve as aggressive a lowering (<120/80 in SPRINT-MIND). This appears to mean that the absolute number or threshold of lowering is potentially less important than the act of lowering the blood pressure from an elevated baseline pressure. Putting this data together with what we have from SPRINT-MIND, it appears that lowering the SBP between 15-20 mmHg in those with an elevated baseline pressure (>140) is probably beneficial in preventing dementia. This kind of adaptive approach enables clinicians to work with individual patients and may help avoid some side effects of aggressive BP lowering in the elderly.
From a prevention standpoint, it almost does not matter why lowering BP is effective in preventing dementia. Does it reduce strokes that can lead to dementia? Does it modulate brain accumulation of amyloid or tau? In my opinion, the next step at the clinical level is to understand if there is a specific class effect for BP lowering that affects progression to dementia. Is this phenomenon more likely with ACEI/ARB drugs, calcium channel blockers or other drugs? This is important because it can and should inform studies of the basic mechanisms behind this relationship between the vascular remodeling resulting from hypertension and how these cascades relate to our understanding of the causes of dementia. We are hoping to identify some of these mechanisms at UCLA in our currently funded NINDS Center Without Walls for Vascular Cognitive Impairment and Dementia.
University of Bristol
In this large-scale, randomized controlled trial, lowering of systolic BP to a mean value of about 130 mmHg and diastolic BP to just below 75 mm Hg was associated with a reduction in all-cause dementia. The cohort included both mid-life and older participants (57 percent in the intervention group and 58 percent in the usual-care group were under 65), and the mean duration for which their hypertension had been documented was eight years.
There is a wealth of data indicating that hypertension is associated with cerebral small-vessel disease, and that the severity of cerebral small-vessel disease increases with the duration of hypertension. The present study did not try to distinguish between the various potential cerebrovascular and neurodegenerative pathological processes that might have contributed to dementia, but over the course of the study there were notably fewer deaths from vascular disease in the intervention group than in the usual-care group (674 versus 832), suggesting that the improved cognitive outcome in the former group was at least partly attributable to reduction in vascular disease.
Observational evidence suggests that there is an association between mid-life hypertension and later-life Alzheimer’s disease (Lennon et al., 2019; Petrovitch et al., 2000; Abell et al., 2018), although the direction of causality remains uncertain.
Particularly in later life, the main mechanism whereby hypertension contributes to dementia seems to be through exacerbation of arteriosclerosis, causing secondary hypoperfusion and blood-brain barrier breakdown; the risk of Alzheimer’s disease may even be reduced (Ruitenberg et al., 2001; Tayler et al., 2023).
References:
Lennon MJ, Makkar SR, Crawford JD, Sachdev PS. Midlife Hypertension and Alzheimer's Disease: A Systematic Review and Meta-Analysis. J Alzheimers Dis. 2019;71(1):307-316. PubMed.
Petrovitch H, White LR, Izmirilian G, Ross GW, Havlik RJ, Markesbery W, Nelson J, Davis DG, Hardman J, Foley DJ, Launer LJ. Midlife blood pressure and neuritic plaques, neurofibrillary tangles, and brain weight at death: the HAAS. Honolulu-Asia aging Study. Neurobiol Aging. 2000 Jan-Feb;21(1):57-62. PubMed.
Abell JG, Kivimäki M, Dugravot A, Tabak AG, Fayosse A, Shipley M, Sabia S, Singh-Manoux A. Association between systolic blood pressure and dementia in the Whitehall II cohort study: role of age, duration, and threshold used to define hypertension. Eur Heart J. 2018 Sep 1;39(33):3119-3125. PubMed.
Ruitenberg A, Skoog I, Ott A, Aevarsson O, Witteman JC, Lernfelt B, van Harskamp F, Hofman A, Breteler MM. Blood pressure and risk of dementia: results from the Rotterdam study and the Gothenburg H-70 Study. Dement Geriatr Cogn Disord. 2001 Jan-Feb;12(1):33-9. PubMed.
Tayler HM, MacLachlan R, Güzel Ö, Miners JS, Love S. Elevated late-life blood pressure may maintain brain oxygenation and slow amyloid-β accumulation at the expense of cerebral vascular damage. Brain Commun. 2023;5(2):fcad112. Epub 2023 Apr 4 PubMed.
Banner Alzheimer's Institute, University of Arizona
This study provides additional randomized trial evidence supporting adequate blood pressure treatment as a strategy to reduce dementia risk. It reinforces that hypertension is common and that public health efforts to address it could have a meaningful impact on dementia prevention.
Notably, the effect size observed was similar to that found in the Systolic Pressure Intervention Trial (SPRINT), although the two trials differ significantly in design. The study does not explore how low blood pressure targets should be, as its goal aligns with the current American Heart Association (AHA) recommendation. However, it underscores the importance of achieving this target, which is often unmet in primary care settings.
The trial also evaluated multiple cardiovascular outcomes (reported in a separate publication), most of which showed that blood pressure control initiated at younger ages offers greater benefits than when started later in life. Future directions include investigating whether lowering blood pressure beyond current AHA recommendations could yield additional benefits, and examining the influence of age on treatment efficacy—for example, whether initiating blood pressure interventions in midlife confers more protection against dementia than starting in older age.
Rush University Medical Center
This work is amazing, as the authors conducted a cluster-randomized clinical trial including 34,000 participants comparing intensive versus usual high blood pressure treatment. I’d like to note several points. The study was not blinded, and the two interventions (the intensive high BP management) and the control (usual high BP management) arms were not balanced. For example, the intervention group received discounted or free antihypertensive medications. This can be a reason for more medication adherence in the intervention group (88.0 percent) vs. the control group (66.4 percent). This may at least partially be responsible for lower dementia incidence in the treatment group together with other factors that are observed in unblinded trials.
Another important point is a trend of effect dilution by advancing age: the risk ratio in favor of intensive BP management was 0.81 in the participants younger than 65, 0.88 in 65-74, and 0.95 in over 75-year-old participants. Although statistically not tested for a trend analysis, the observed trend suggests that intensive BP management may not be useful for the oldest old who are at the highest risk of dementia. Similarly, the possible side effects of intensive antihypertensive treatment (such as serious falls) are not reported by age group, which may be the most severe in the oldest group.
My conclusion is that while the study supports intensive antihypertensive treatment in younger hypertensive patients, finding the cut-point for antihypertensive treatment in the oldest old patients for the prevention of dementia needs more trials.
Make a Comment
To make a comment you must login or register.