Plaque Removal Delays Onset of Familial Alzheimer’s Disease
Quick Links
The first evidence that removing amyloid plaques may delay Alzheimer’s symptoms has now been published. In The Lancet Neurology on March 19, scientists led by Randall Bateman at Washington University in St. Louis described findings from the open-label extension of the Dominantly Inherited Alzheimer Network Trials Unit’s first prevention study. For cognitively healthy people who carried an autosomal dominant AD mutation, eight years of treatment with gantenerumab halved the odds of developing symptoms. A preliminary analysis was presented at the 2024 Alzheimer’s Association International Conference (Aug 2024 conference news). The paper adds details and safety data.
- On gantenerumab, autosomal-dominant AD mutation carriers halved their odds of developing symptoms.
- This occurred even though plaques did not fully disappear.
- These patients are now enrolled in an open-label follow-up with lecanemab.
- This will test if eliminating plaque can keep symptoms at bay or slow decline.
The first secondary prevention trial in the DIAN cohort, known as DIAN-TU-001, enrolled 144 mutation carriers, who received gantenerumab, solanezumab, or placebo for an average of five years. The trial included people with and without symptoms, and did not detect a cognitive benefit for either group. However, because gantenerumab whittled away at plaques and curbed p-tau181 and total tau in cerebrospinal fluid, DIAN researchers offered participants a two-year open-label extension of high-dose gantenerumab (Feb 2020 news; Apr 2020 conference news).
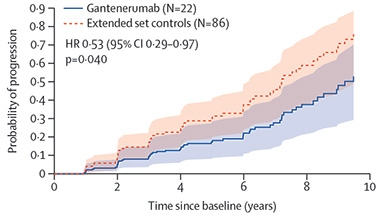
Delaying the Disease. People who took gantenerumab (blue) for eight years had half the odds of developing symptoms as did controls (red). [Courtesy of Bateman et al., Lancet Neurology, 2025.]
About half of the original participants, who’d received either placebo or immunotherapy, enrolled in the OLE. The group tilted toward those who had been symptom-free at trial baseline, because many symptomatic participants had declined too much to continue treatment. Of the 73 OLE participants, 53 had been cognitively healthy at the beginning of the placebo-controlled trial and stayed in the OLE long enough to be included in the analysis. This group was slightly less likely to develop symptoms than were untreated ADAD controls, with a hazard ratio of 0.84, but the difference was not statistically significant.
However, only 22 had taken gantenerumab from the get-go, i.e., during the placebo-controlled trial as well as in the OLE. For this smaller group, with an average of 8.4 years of gantenerumab exposure, the odds of declining on the CDR-SB were about half that of people who’d never been on the immunotherapy (image above). The difference was nominally significant at p=0.04. This longest-treated group also had about half the odds of clinical worsening on the MMSE and the Functional Assessment Scale, though these protections missed statistical significance.
The authors noted that the finding of 50 percent slower disease progression was robust, being unchanged after controlling for multiple factors, for example by using controls matched to each participant’s estimated year of onset and mutation type. In addition, they reported that in the placebo-controlled portion of the trial, cognitively healthy participants on gantenerumab were half as likely to develop symptoms as were those on solanezumab or placebo, though this again missed significance.
Now on to the safety of the treatment. In the OLE, participants received 1,500 mg gantenerumab twice monthly, about triple the 1,020 mg monthly dose given in the placebo-controlled DIAN-TU trial and in the Graduate 1 and 2 Phase 3 trials of gantenerumab in late-onset sporadic AD. The lower dose had failed to completely clear plaque in people with autosomal dominant AD, who accumulate amyloid rapidly. The high OLE doses caused 50 percent more ARIA-E, with incidence rising from 20 to 30 percent. This is similar to what was seen in Phase 3 trials of gantenerumab and donanemab in sporadic AD. In the DIAN-TU OLE, six out of 32 ARIA-E episodes caused symptoms such as headaches and disorientation; two participants were hospitalized and later recovered.
Similarly, ARIA-H events were more common in the OLE, with the incidence of microhemorrhages almost doubling from 24 to 47 percent, and superficial siderosis rising from 4 to 7 percent. Both ARIA-E and -H were more common in symptomatic than asymptomatic participants, likely due to their higher plaque load (Joseph-Mathurin et al., 2021; Joseph-Mathurin et al., 2022).
Despite the increase in ARIA, there were half as many other serious adverse events related to treatment, such as nervous system disorders. These dropped from 23 percent in the trial to 12 percent in the OLE. There were no macrohemorrhages or deaths due to ARIA.
Notably, even the very high gantenerumab doses used in the OLE did not fully clear plaque in most participants. Average plaque load dropped from 62 to 33 centiloids, which is above the amyloid-positivity threshold of 24. Of the 55 OLE participants with PiB PET data, 38 people, or about two-thirds, remained amyloid-positive. Among the subgroup with eight years of gantenerumab exposure, about a quarter remained amyloid-positive. Former OLE participants are now enrolled in the Amyloid Removal Trial, an open-label study of lecanemab that will evaluate the effects of fully removing plaque on disease progression and downstream biomarkers in this group (Aug 2024 conference news).—Madolyn Bowman Rogers
References
News Citations
- Living Among Us: People Whose Alzheimer’s Is Already Being Prevented
- Topline Result for First DIAN-TU Clinical Trial: Negative on Primary
- In DIAN-TU, Gantenerumab Brings Down Tau. By a Lot. Open Extension Planned
- First Success Stories From Alzheimer’s Secondary Prevention Trial
Therapeutics Citations
Paper Citations
- Joseph-Mathurin N, Wang G, Kantarci K, Jack CR Jr, McDade E, Hassenstab J, Blazey TM, Gordon BA, Su Y, Chen G, Massoumzadeh P, Hornbeck RC, Allegri RF, Ances BM, Berman SB, Brickman AM, Brooks WS, Cash DM, Chhatwal JP, Chui HC, Correia S, Cruchaga C, Farlow MR, Fox NC, Fulham M, Ghetti B, Graff-Radford NR, Johnson KA, Karch CM, Laske C, Lee AK, Levin J, Masters CL, Noble JM, O'Connor A, Perrin RJ, Preboske GM, Ringman JM, Rowe CC, Salloway S, Saykin AJ, Schofield PR, Shimada H, Shoji M, Suzuki K, Villemagne VL, Xiong C, Yakushev I, Morris JC, Bateman RJ, Benzinger TL, Dominantly Inherited Alzheimer Network. Longitudinal Accumulation of Cerebral Microhemorrhages in Dominantly Inherited Alzheimer Disease. Neurology. 2021 Mar 23;96(12):e1632-e1645. Epub 2021 Jan 25 PubMed.
- Joseph-Mathurin N, Llibre-Guerra JJ, Li Y, McCullough AA, Hofmann C, Wojtowicz J, Park E, Wang G, Preboske GM, Wang Q, Gordon BA, Chen CD, Flores S, Aggarwal NT, Berman SB, Bird TD, Black SE, Borowski B, Brooks WS, Chhatwal JP, Clarnette R, Cruchaga C, Fagan AM, Farlow M, Fox NC, Gauthier S, Hassenstab J, Hobbs DA, Holdridge KC, Honig LS, Hornbeck RC, Hsiung GR, Jack CR Jr, Jimenez-Velazquez IZ, Jucker M, Klein G, Levin J, Mancini M, Masellis M, McKay NS, Mummery CJ, Ringman JM, Shimada H, Snider BJ, Suzuki K, Wallon D, Xiong C, Yaari R, McDade E, Perrin RJ, Bateman RJ, Salloway SP, Benzinger TL, Clifford DB, Dominantly Inherited Alzheimer Network Trials Unit. Amyloid-Related Imaging Abnormalities in the DIAN-TU-001 Trial of Gantenerumab and Solanezumab: Lessons from a Trial in Dominantly Inherited Alzheimer Disease. Ann Neurol. 2022 Nov;92(5):729-744. Epub 2022 Oct 13 PubMed.
Further Reading
News
- In ADAD, Plaque Removal Improves Synaptic and Inflammatory Biomarkers
- Treat Before ‘Aβ Bothers Tau,’ Scientists Say at CTAD
- Is It Time to Approve Drugs Based on Amyloid Removal?
- Gotta Get Rid of It All: Total Plaque Clearance Key for Clinical Benefit
- What Happens After Amyloid Plaque Removal? Who Benefits Most?
- Scientists Ask What Plaque Clearance Means for the Long Haul
- Gantenerumab Mystery: How Did It Lose Potency in Phase 3?
Primary Papers
- Bateman RJ, Li Y, McDade EM, Llibre-Guerra JJ, Clifford DB, Atri A, Mills SL, Santacruz AM, Wang G, Supnet C, Benzinger TL, Gordon BA, Ibanez L, Klein G, Baudler M, Doody RS, Delmar P, Kerchner GA, Bittner T, Wojtowicz J, Bonni A, Fontoura P, Hofmann C, Kulic L, Hassenstab J, Aschenbrenner AJ, Perrin RJ, Cruchaga C, Renton AE, Xiong C, Goate AA, Morris JC, Holtzman DM, Snider BJ, Mummery C, Brooks WS, Wallon D, Berman SB, Roberson E, Masters CL, Galasko DR, Jayadev S, Sanchez-Valle R, Pariente J, Kinsella J, van Dyck CH, Gauthier S, Hsiung GR, Masellis M, Dubois B, Honig LS, Jack CR, Daniels A, Aguillón D, Allegri R, Chhatwal J, Day G, Fox NC, Huey E, Ikeuchi T, Jucker M, Lee JH, Levey AI, Levin J, Lopera F, Roh J, Rosa-Neto P, Schofield PR, Dominantly Inherited Alzheimer's Disease–Trials Unit. Safety and efficacy of long-term gantenerumab treatment in dominantly inherited Alzheimer's disease: an open-label extension of the phase 2/3 multicentre, randomised, double-blind, placebo-controlled platform DIAN-TU trial. Lancet Neurol. 2025 Apr;24(4):316-330. PubMed.
Annotate
To make an annotation you must Login or Register.
Comments
No Available Comments
Make a Comment
To make a comment you must login or register.