First Glimmers of Lecanemab Efficacy in the “Real World”?
Quick Links
The therapeutic antibody lecanemab has been in clinical use in the U.S. for two years, and doubts about whether it would be feasible for clinics to implement and manage this therapy have eased. Even so, a burning question remains: Does the treatment work? At the Alzheimer’s Association International Conference, held July 27-31 in Toronto, speakers offered perhaps the first hints of efficacy in routine clinical practice, a.k.a. “real world” in medical lingo.
- Some patients on lecanemab declined more slowly than expected based on individualized disease trajectories.
- In China, lecanemab patients did better after six months than matched controls.
- A U.S. study found most lecanemab patients remained clinically stable for a year.
Christopher Brown at the University of Pennsylvania, Philadelphia, described how he used individualized clinical trajectories to determine whether an Alzheimer’s patient was worsening more slowly than would be expected. For the first 23 people at his site to reach a year of treatment, this method pointed toward a statistically significant slowing of clinical decline. It also flagged nonresponders. One attendee called the data remarkable, and many expressed interest in the method.
Scientists at Peking Union Medical College Hospital in Beijing, a.k.a. PUMCH, presented similar data. They compared 29 patients on lecanemab with matched controls. In Toronto, they reported consistent trends toward slower cognitive and functional decline after six months of treatment. Other speakers presented interim data from an Eisai post-market study of lecanemab that found 87 percent of patients remained clinically stable after a year, a tad more than would be expected based on natural history studies.
In all these studies, patient numbers are tiny, and the findings lack placebo controls. Nonetheless, sessions on real-world lecanemab use packed large lecture halls at AAIC, with attendees asking questions until the time ran out.

Altered Fate? Modeling predicts (left, open circles) a person’s cognitive worsening (y axis) as their tau pathology accumulates (x axis). Some people are vulnerable (pink), i.e., worsening faster than normal, some follow a typical AD time course (aqua), and some are resilient (yellow). After a year on lecanemab (right), most patients are doing better than predicted, as seen in the divergence between the open circle and second solid circle. [Courtesy of Christopher Brown, University of Pennsylvania.]
Personalized Predictions
Small increments of possible efficacy are hard to detect in clinical practice. There are no controls, and disease progression varies from one person to another. To solve this problem, Brown turned to algorithms developed by Tobey Betthauser at the University of Wisconsin, Madison. Betthauser works on amyloid and tau “clocks,” and recently described a statistical method for using a person’s tau PET scan to determine when that person first became positive, i.e., their “tau time” (Heston et al., 2025). Brown adapted the algorithm for use with a different tau biomarker, plasma p-tau217, which is more readily available in clinical practice (Brown et al., 2025).
Next, Brown used tau time and cognitive scores to determine whether given patients were worsening at a faster or slower rate than normal. The recently updated AD diagnostic criteria align clinical stages with the spatial extent of tau pathology. They define vulnerable people as those who have more clinically advanced disease than expected based on their tau stage, and resilient people as those who are cognitively healthier than expected (Aug 2023 conference news).
Brown applied this concept to longitudinal datasets from ADNI and the UPenn Alzheimer’s Disease Research Center. He found that about half of Alzheimer’s patients had a mismatch between their tau time and CDR-SB score that indicated they were either vulnerable or resilient (image below). As predicted, the former group declined quickly, the latter slowly (Brown et al., 2025).
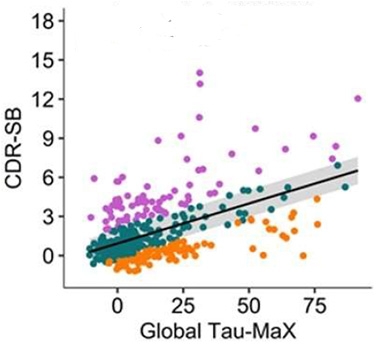
Finding Mismatches. In AD cohorts, vulnerable people (pink) decline faster than expected based on their tau pathology, while resilient people (yellow) worsen more slowly than expected. [Courtesy of Brown et al., medRxiv, 2025.]
This tool enabled Brown to forecast individualized trajectories for people on amyloid immunotherapy based on their plasma p-tau217, CDR-SB score, and the degree of mismatch between where each patient was compared with the expected time course of AD decline. His model also includes variables such as age, sex, and education, which improved predictive accuracy.
Detecting Change in Clinical Practice
At UPenn, Brown leads the Anti-Amyloid Therapy (AAT) Monitoring Study, which tracks people on lecanemab. Participants give blood monthly and take cognitive assessments twice a week using a mobile app. They also come to the clinic every six months to take standard clinical tests, including the MMSE and the Dementia Severity Rating Scale. Brown noted that MMSE and DSRS scores can be transformed into CDR-SB scores with high accuracy.
In Toronto, Brown reported early findings from this study. For 43 people on lecanemab, combining their individualized trajectories predicted that without treatment, the cohort’s plasma p-tau217 would remain stable over three months. Instead, plasma p-tau217 dropped. The improvement in plasma p-tau217 was similar to that seen in the Phase 3 trial of donanemab, Brown noted. He used this trial as a comparator because the Clarity Phase 3 trial of lecanemab did not include a three-month timepoint for this biomarker.
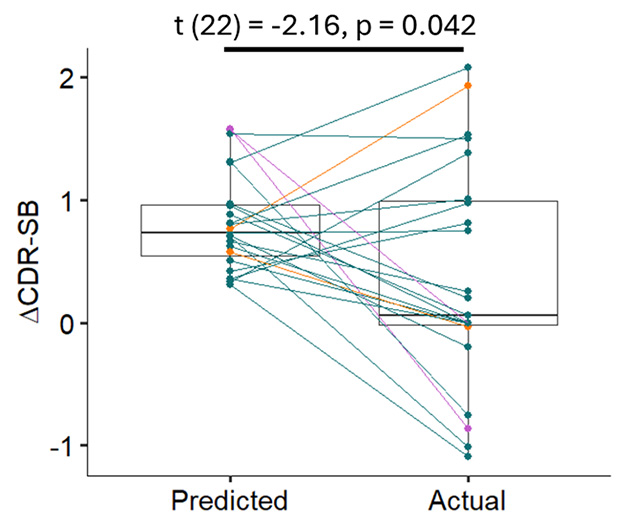
See a Benefit? Spaghetti plot shows each AD patient’s predicted CDR-SB after a year (left), compared with their actual scores after a year on lecanemab (right). [Courtesy of Christopher Brown, University of Pennsylvania.]
What about cognition? So far, 23 patients have reached one year of treatment. Brown compared their cognitive change to what would be expected based on their individualized predictions. He showed spaghetti plots of each person’s expected and actual trajectories. Most of the latter had either worsened more slowly than predicted, or improved slightly (image at top of story). For the cohort overall, CDR-SB scores stayed nearly flat on lecanemab, compared with a predicted worsening of about three-quarters of a point (image above). The findings were statistically significant at p=0.04.
Six nonresponders continued to worsen cognitively. In future work, Brown plans to run proteomic analyses of baseline plasma to identify factors that could predict a person’s response to immunotherapy.
Other speakers in Toronto offered preliminary data on this point from their practices. David Weisman at Abingdon Neurology Associates, Pennsylvania, noted that in his experience, older patients do better on immunotherapy than younger ones, perhaps because they have less tau pathology on average. Larry Honig at Columbia University, New York City, presented an analysis of the 239 lecanemab patients there. Those who started with an MMSE of 24 or higher improved two points on average over two years of treatment, while those with baseline MMSEs of 23 or less declined three points. Accumulating data suggests people at earlier disease stages derive more benefit from amyloid immunotherapy (Nov 2023 conference news).
An attendee asked how feasible it is to add Brown’s AAT Monitoring Study protocol to one’s clinical practice. Brown said they picked tests that were simple and quick to administer. In addition to blood draws and mobile cognitive testing, the study also adds several sequences to standard MRI monitoring scans to help determine how the drug affects fluid in the brain, including ARIA changes. Brown said those data are preliminary, and he will present them at a later conference.
Similar in China
In Toronto, Wenjun Wang at Beijing’s PUMCH reported findings from their cohort. The analysis was led by senior author Jing Gao and first author Chenhui Mao. Wang noted that lecanemab has been used in China for a year, and PUMCH serves 31 provinces, drawing patients from a wide catchment area. Few people are on lecanemab just yet, and Wang reported six months of data from 29 patients. All were amyloid-positive, with MCI or mild dementia. They were 66 years old on average, almost two-thirds were female, and almost two-thirds carried an E4 allele—in other words, a typical if young AD cohort.
At baseline, these patients had 59 centiloids of plaque on average. After six months, they had cleared an average of 31 centiloids, nearly identical to the 33 centiloids cleared in that time in Clarity. Three nonresponders continued to accumulate plaque, one didn’t change. On fluid biomarkers, plasma Aβ42/40 and GFAP improved, while p-tau181 and p-tau217 remained flat.
When compared with matched controls from PUMCH, people on lecanemab for six months declined numerically less on the CDR-SB and MMSE, and on activities of daily living. Individual variation was large, and the findings missed statistical significance. Wang did not specify how matched controls were chosen. These presenters did not respond to Alzforum’s request for image permission, hence this story refrained from showing any.
Eisai Study Reports Clinical Stability
The Eisai study likewise reported a whiff of clinical benefit. This study involves 15 clinical sites, with final results expected this coming winter. In Toronto, scientists reported interim data from nine sites and 177 patients. They were 74 years old on average; 58 percent of them had MCI, the rest mild dementia. Two-thirds were APOE4 carriers, including 18 percent who were homozygotes. Overall, they have been taking lecanemab for close to a year, and 87 percent of them remain in the study.
Weisman went over the clinical findings. At six months, 87 percent of patients had not progressed to a later disease stage, including 6 percent who improved from mild dementia to MCI. The numbers were nearly identical at 10 months, the average length of treatment in this cohort at the time data were analyzed.
Only 15 people have reached 18 months of treatment. Among them, 87 percent had not worsened, and 20 percent had improved from mild dementia to MCI. If these trends hold for the whole cohort, about 70 percent would be expected to be stable or improved at 18 months based on the survival curves, Weisman calculated. He noted the confidence interval at this time point was broad, with estimates ranging from 55 to 80 percent. Overall, he said the cohort has worsened by about one point on the MoCA and MMSE, and two points on the FAQ, over slightly more than a year of treatment. He called this minimal change.
Weisman did not compare the findings with data from observational trials. An audience member noted that 80 to 90 percent of people with clinical MCI typically remain stable over a year. Co-chair Babak Tousi at the Cleveland Clinic in Ohio said that people with biomarker-confirmed AD progress faster. One study from the National Alzheimer’s Coordinating Center found that 78 percent of people with biomarker-confirmed MCI-AD, and 64 percent of people with mild AD, did not worsen over a year (Potashman et al., 2021). Given that the Eisai cohort was 58 percent MCI, those rates would translate to about 72 percent remaining stable for a year, a bit lower than the reported 87 percent. In Clarity, 75 percent of the placebo group remained stable on the CDR for a year, and 68 percent for 18 months.
How do patients feel about treatment? Anecdotal reports at AAIC suggest that many are enthusiastic. Honig noted that patients and family members at his clinic tend to keep their clinical appointments, hew closely to treatment guidelines, and remain on drug. Suzanne Schindler at Washington University, St. Louis, said that many of her patients have made social connections, for example finding “infusion buddies” who go with them to treatments. Michael Rosenbloom at the University of Washington, Seattle, noted that depression lightens over time in his patients, and speculated that it could be due to these patient support groups. How much these social connections factor into clinical stability remains unknown.—Madolyn Bowman Rogers
References
Therapeutics Citations
News Citations
- Revised Again: Alzheimer's Diagnostic Criteria Get Another Makeover
- Treat Before ‘Aβ Bothers Tau,’ Scientists Say at CTAD
Paper Citations
- Heston MB, Teague JP, Cody KA, Deming Y, Ruiz de Chavez E, Morse J, Chin NA, Engelman CD, Chappell RJ, Langhough RE, Gleason CE, Clark LR, Zuelsdorff ML, Betthauser TJ, Alzheimer’s Disease Neuroimaging Initiative. Factors associated with age at tau pathology onset and time from tau onset to dementia. medRxiv. 2025 Mar 13; PubMed.
- Brown CA, Das SR, Cousins KA, Tropea TF, Plotkin AC, Detre JA, Yushkevich PA, McMillan CT, Lee EB, Shaw LM, Nasrallah IM, Alzheimer's Disease Neuroimaging Initiative, Wolk DA. Tau burden is best captured by magnitude and extent: Tau-MaX as a measure of global tau. Alzheimers Dement. 2025 Jul;21(7):e70346. PubMed.
- Brown CA, Mundada NS, Cousins KA, Sadeghpour N, Lyu X, McGrew E, Korecka M, Chen-Plotkin A, Xie L, Wisse LE, Detre JA, McMillan CT, Lee EB, Nasrallah IM, Das SR, Mechanic-Hamilton D, Yushkevich PA, Shaw LM, Alzheimer’s Disease Neuroimaging Initiative, Wolk DA. Tau-Clinical Mismatch Identifies Individuals with Co-Pathology and Predicts Clinical Trajectory. medRxiv. 2025 Jul 25; PubMed.
- Potashman M, Buessing M, Levitchi Benea M, Cummings J, Borson S, Pemberton-Ross P, Epstein AJ. Estimating Progression Rates Across the Spectrum of Alzheimer's Disease for Amyloid-Positive Individuals Using National Alzheimer's Coordinating Center Data. Neurol Ther. 2021 Dec;10(2):941-953. Epub 2021 Aug 24 PubMed.
Further Reading
News
Annotate
To make an annotation you must Login or Register.
Comments
Abington Neurological
There will never be better datasets than the Phase 2 and 3 RCTs of anti-amyloid therapies. We should look to these studies to inform clinical practice. We will have more trials from other anti-amyloid drugs, and the prevention trials will result in a couple of years or so, which I think will likely further support the drug class.
It is still good to learn the lessons our patients teach us. While the clinical picture is obviously confounded by placebo and nocebo effects, test-retest, and the symptomatics, treating clinicians are still getting an intuitive feel for these drugs. And the feeling is good. I've seen firsthand not just the hope these drugs offer on the first infusion day, but the fact that some patients respond very well. I just had two consecutive patients who have less functional impairment and better testing compared with their baseline. Wish I could predict this, but they MOSTLY seem to be milder with typical amnestic disease.
The practical application of these drugs, not getting burned by severe ARIA, and observing these favorable clinical effects leaves me more enthusiastic now than in 2022-23 with the Clarity results and our first clinical dose.
Make a Comment
To make a comment you must login or register.