Signs of Lasting Benefit From Amyloid Immunotherapy?
Quick Links
With two amyloid immunotherapies on the market in many countries, scientists are eager for information on how durable their clinical effects will be. At this year’s Alzheimer’s Association International Conference, held July 27-31 in Toronto, speakers offered a glimpse. Four-year open-label extension data for lecanemab, and three-year OLE data for donanemab, appeared to show the clinical benefit widening over time when compared with matched controls from longitudinal observational studies of Alzheimer’s disease.
- After four years on lecanemab, the numerical clinical benefit tripled.
- People who started with almost no tangles did best, with half improving over baseline.
- After three years, the initial donanemab benefit doubled.
People at earlier disease stages did best, a consistent finding in trials of these drugs. Among those who started with few tangles in their brains, two-thirds had not declined after four years; indeed, more than half improved on cognitive and functional tests. As with all open-label data, the findings need to be interpreted cautiously. This is due to the lack of placebo controls and to attrition bias, whereby many of those who drop out are lost to follow-up.
“This durable and increasing benefit indicates a disease-modifying effect that further supports removing amyloid in early stages,” Randall Bateman of Washington University, St. Louis, wrote to Alzforum. In the future, he would like to see data on whether long-term treatment delays outcomes such as disability, nursing home placement, and death. Philip Scheltens of EQT Life Sciences, Amsterdam, co-chaired the session. He found it encouraging that many people stayed on immunotherapy for years, even though this required them to get biweekly or monthly infusions. “All in all, the data showed good progress on long-term safety and efficacy,” Scheltens wrote.
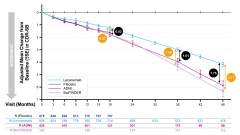
Watching the Gap. At 18 months, lecanemab (blue) lifted CDR-SB performance by about half a point (black circle) over that of matched ADNI participants (magenta). At 36 months, this difference doubled, and by 48, it tripled. Against matched BioFinder1 participants (lavender), differences were slightly greater (orange circles). [Courtesy of Eisai.]
Long-Term Lecanemab Data Support Disease-Modifying Effect
The findings match earlier reports. At the 2024 AAIC, Chris van Dyck of Yale School of Medicine in New Haven, Connecticut, presented 18-month OLE data from the Clarity Phase 3 study. For people who had been on lecanemab during the trial, this meant they had had three years of continuous treatment. When compared to matched controls from ADNI, at that point they scored 0.95 points better on the CDR-SB. This is about twice the 0.45 benefit over placebo measured at the end of the 18-month controlled trial period. In addition, people treated for three years maintained an advantage over those who switched from placebo and thus had spent only 18 months on drug (Aug 2024 conference news).
In Toronto, van Dyck updated these numbers and added four-year treatment data. Calculating the difference between the treatment group and ADNI controls at each time point, and including additional Clarity participants who reached 36 months of treatment, the treatment effect was 0.52 points at 18 months and 1.01 at 36 months, he said. By four years, the CDR-SB difference had widened to 1.75 points, more than three times the initial benefit. Because a matched control group from a separate observational study is less reliable than placebo controls in the trial, the scientists tested the robustness of the findings against a second observational study, Biofinder 1. These participants all started with mild cognitive impairment, and thus had less advanced disease on average than Clarity participants, a third of whom had mild dementia. Nonetheless, the Clarity cohort notched a bigger advantage versus Biofinder 1, amounting to 0.57 points at 18 months, 1.4 at three years, and 2.17 at four years (image above).
Noting that people who remain in open-label studies tend to be healthier, an audience member asked if Eisai had analyzed differences between remaining participants and the whole cohort. Van Dyck said he had not seen such an analysis, but noted that the same attrition effect afflicts longitudinal studies like ADNI and Biofinder 1. After four years the lecanemab group had dropped from 859 to 478 people, an attrition rate of 44 percent, while the matched ADNI controls dropped from 436 to 98 people, an attrition of 78 percent.
While clinical scores provide a benchmark, what patients really care about is how fast their disease worsens. Here, too, the lecanemab data suggest a long-term benefit. At three years, Clarity participants were 30 percent less likely to have deteriorated to the next stage of disease than were people in ADNI. This advantage was maintained at four years, when the Clarity cohort was 34 percent less likely to have worsened than were ADNI controls. Overall, at the four-year timepoint, almost half of continuously treated Clarity participants remaining in the trial had stayed at their baseline disease stage.
In terms of healthy time gained, the Clarity group had an advantage of five months over ADNI participants at 18 months, and this lengthened to 10.7 months at four years. Comparing Clarity with Biofinder 1, the differences were 5.5 and 13.1 months, respectively.
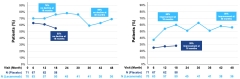
Disease Arrested? Of the participants who started the Clarity trial with very low tau, a greater proportion stabilized (left) or improved (right) on lecanemab (light blue) at timepoints up to four years. Dark blue shows those who stayed stable or improved on placebo. [Courtesy of Eisai.]
The Earlier, the Better
Data from multiple studies have slowly bolstered the idea that starting amyloid immunotherapy early in disease, before tangles take off, brings bigger benefits (Nov 2023 conference news). Clarity participants who started with few tangles, i.e., a tau PET SUVR below 1.06, were the most likely to remain stable on lecanemab. At 18 months, three-quarters of low-tau participants on lecanemab had not declined on the CDR-SB; 60 percent had improved. This contrasted with 55 and 28 percent, respectively, for the untreated low-tau group. At three years, 59 percent of people on lecanemab had not declined, and 51 percent had improved. There was no comparator group at this timepoint. In addition, the numbers were small: 50 people at 18 months, and 41 at three years.
By four years, five more people had dropped out, leading to slighter higher numbers for the 36 people remaining—69 percent had not declined, and 56 percent had improved over baseline (image above). For contrast, in the whole Clarity cohort, 47 percent remained stable on lecanemab for four years. Bateman asked what these data mean for prevention efforts. “We should go as early as possible,” van Dyck said.

Consistent Pattern. On donanemab (red), the initially small clinical benefit at 18 months had doubled at three years compared with matched ADNI controls (blue). [Courtesy of Eli Lilly.]
Different Drug, Same Picture
In Toronto, Mark Mintun of Eli Lilly showed similar data for donanemab. The Trailblazer-Alz2 Phase 3 trial started after Clarity, hence its OLE data go only to three years thus far. As with lecanemab, Lilly scientists used matched ADNI participants as controls. The data looked nearly identical, where treatment benefit doubled from 18 to 36 months, going from 0.6 to 1.2 points on the CDR-SB. As in Clarity, about half the participants had dropped out by three years. The donanemab group went from 794 to 417 people, an attrition of 47 percent, while ADNI controls dropped from 268 to 122 people, or 55 percent (image above).
At three years, people on donanemab ran 27 percent less risk of progressing to the next stage of their disease than did ADNI controls, similar to the 30 percent reported for Clarity participants at this time point. However, Lilly scientists were unable to analyze low-tau participants, since having tangles was an inclusion criterion and no one in the cohort was below 1.06 SUVR. The company is studying a low-tau group in its ongoing prevention trial, Trailblazer-Alz3 (Nov 2024 conference news).
What about people who switched from placebo to drug after 18 months? Mintun noted that about half of this group had progressed to moderate dementia before the OLE began. Nonetheless, they still appeared to reap some benefit, scoring 0.8 points better on the CDR-SB at the three-year timepoint than did ADNI controls.
Another point of convergence between lecanemab and donanemab was that ARIA-E dropped to background levels during the OLE for both, consistent with previous findings that ARIA risk is highest in the first six months to one year of treatment.
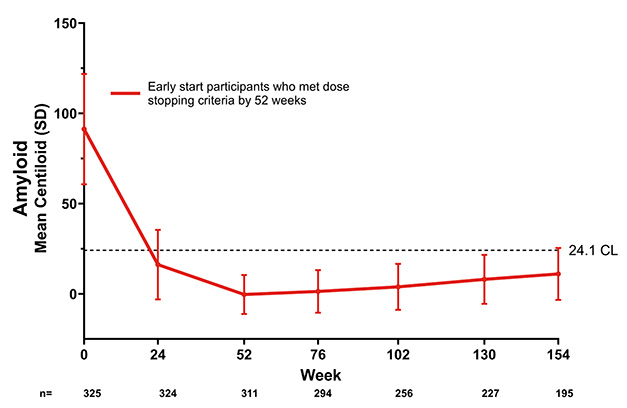
Get Out, Stay Gone. People who became amyloid-negative by one year on donanemab remained below the PET positivity threshold (dotted line) two years later. [Courtesy of Eli Lilly.]
Keep Treating or Stop?
Despite these similarities, one difference looms large between lecanemab and donanemab. In the Clarity OLE, everyone stays on drug, because trial data show that fluid biomarkers rapidly rebound without treatment (Mar 2022 conference news). In the Trailblazer-Alz2 OLE, most were off donanemab. During both the controlled phase of this trial and the OLE, participants were switched to placebo infusions when they became amyloid-negative. In other words, about 70 percent of participants took placebo, not donanemab, for the entire 18 months of the OLE, Mintun said. Plaque re-accumulated at 2.5 centiloids per year, about the rate seen in natural disease progression (image above). Lilly scientists did not show fluid biomarker data from donanemab’s open-label trial in Toronto.
To scientists at AAIC, it remained a conundrum why one antibody requires continued dosing, while the other apparently does not. They do have different targets, with lecanemab preferentially targeting Aβ protofibrils, and donanemab recognizing a sticky, pyroglutamated form of Aβ found only in plaques. Still, both antibodies remove plaques to below the brain-wide threshold of positivity. Many researchers don’t know what to make of the difference.
In Toronto, an audience member asked if donanemab dosing should really stop. Mintun said the OLE data are not yet definitive enough to make a clinical recommendation. Meanwhile, John Sims at Lilly has said the company will test a maintenance dose of donanemab in its Trailblazer-Alz3 study of preclinical AD. Because this group is likely to live the longest with AD, he believes it is the best population in which to study continued dosing (Endpoints news).—Madolyn Bowman Rogers
References
Therapeutics Citations
News Citations
- Leqembi: The Case for Long-Term Dosing
- Treat Before ‘Aβ Bothers Tau,’ Scientists Say at CTAD
- Fully Loaded: Secondary Prevention Studies of Lecanemab, Donanemab
- Using Lecanemab Trial Data to Determine Maintenance Dose
External Citations
Further Reading
Annotate
To make an annotation you must Login or Register.
Comments
Henan Academy of Innovations in Medical Science
Is this not just some statistical artefact where the worst cases drop out and the overall group appears to have improved? And aren’t all patients getting worse and die? Is this the treatment we all have been waiting for?
Laval University Research Center
To show disease modification, we need to follow the placebo who switched to the drug. A true disease-modifying effect is demonstrated when patients with a late start (placebo-drug) never catch up to those with an early start (drug-drug). With donanemab, there was another slide showing a difference of 0.8 for the switchers (instead of 1.2 on CDR-SB), which is thus consistent with disease modification. I know it sounds counterproductive, but that’s what disease modification means: you need to start early to gain on the long term. You cannot ever fully recover from the 18-month placebo.
University of Sydney
I think Christian does have a point. From the data there was a huge reduction in amyloid, but the overall trend is similar. There must be more things going on that are beyond solely targeting Aβ. Dare I say, it may even be beyond targeting Aβ and tau.
That being said, there are cancer patients who do everything they can extend their lives six to 12 months. I wonder if it is ever possible to flatten the line in the future or if it is a rather incurable disease like glioblastoma, which spreads far too infiltratively in healthy white matter. I think collectively there need to be more risks taken in trying different combination approaches, but am not sure—perhaps adding treatment complexity is also cost prohibitive?
Make a Comment
To make a comment you must login or register.