Microtuble-Binding Region—the Next Marker for Immunoassay Platforms?
Quick Links
Phospho-tau217 has emerged as an excellent marker of the presence of amyloid pathology in the brain, but for markers of neurofibrillary tangles, fragments of tau’s microtubule binding region have a leg up. Clinics may soon be able to detect these MTBR fragments on commercial immunoassay platforms. At AAIC in Toronto last month, scientists led by Kaj Blennow at the University of Gothenburg, Mölndal, Sweden, introduced two new immunoassays for MTBR, dubbed MTBR1 and MTBR-p262. The latter only binds to fragments containing a phospho group on amino acid 262.
- CSF MTBR-243, detected by mass spectroscopy, tracks with tangles.
- New antibodies detect similar fragments in CSF.
- These correlate with tangles but also with neurodegeneration.
- MTBR-243 may specifically recognize 3R/4R isoforms of tau.
Both assays detect fragments containing an epitope in the first microtubule-binding repeat. Both seem to track with tau pathology. For now, the assays work well for cerebrospinal fluid. Blennow told Alzforum he hopes to get them working in plasma, adding that several companies are interested in developing them commercially. The caveat: MTBR1 renders high values not only from people with Alzheimer’s, but also Creutzfeldt-Jacob disease, suggesting it may be a marker of neurodegeneration.
Previous work from Kanta Horie and colleagues at Washington University, St. Louis, indicated that MTBR-243 in the CSF, and eMTBR-tau243, a fragment of the MTBR region that can be detected in plasma, are better markers for tangles than any of the various phospho-tau fragments, which begin to climb in blood before tau PET scans turn positive (Apr 2025 conference news). In Toronto, these scientists reported that eMTBR-243 specifically recognizes tangles containing a mixture of three-repeat and four-repeat tau isoforms, such as those found in AD and chronic traumatic encephalopathy.
Horie and colleagues use mass spectrometry to measure these fragments, but most clinics do not have mass spectrometers. Could an immunoassay work equally well?
To this end, Fernando Gonzalez-Ortiz in Blennow’s lab collaborated with scientists at Bioventix. This biotech company in Farnham, England, specializes in generating sheep antibodies for diagnostics. Companies then license its antibodies to create assays on their respective diagnostic platforms. Besides having generated an antibody that recognizes isoforms of tau only made in the brain (Dec 2022 conference news), Bioventix generated antibodies that cover many regions of tau, including those that span the MTBR.
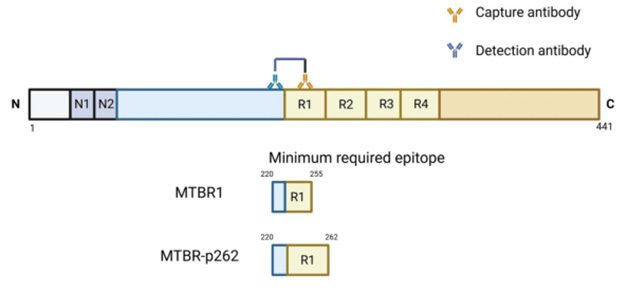
New Strategy. MTBR1 detects tau fragments containing amino acids 220-255. MTBR-p262 binds fragments that contain a longer epitope, with position 262 phosphorylated. [Courtesy of Fernando Gonzalez-Ortiz, University of Gothenburg.]
In Toronto, Gonzalez-Ortiz reported on two SIMOA-based immunoassays using such antibodies. MTBR1 detects a non-phosphorylated epitope between amino acids 220 and 255, covering most of the first microtubule-binding repeat. MTBR-p262 identifies an epitope in the 220-262 fragment that is phosphorylated on the C -terminus (image above).
The UGoth scientists tested MTBR1 in CSF samples from three cohorts: the Norwegian Dementia Disease Initiation (DDI) study, which includes people who are cognitively normal or have very early AD; a cohort from a memory clinic in Copenhagen, Denmark; and a pilot study from Lund University that is part of a Gates Ventures initiative to study biomarkers in AD and related neurodegenerative diseases. The initiative includes amyloid and tau PET. This cohort is unpublished, Gonzalez-Ortiz said, but he has been using it as a pilot study for the new MTBR immunoassays.
In DDI, MTBR1 differentiated 84 people who were amyloid-negative and cognitively stable from 125 who were amyloid-positive. Some of the latter had mild cognitive impairment and some were cognitively normal. MTBR1 did not distinguish between these two groups. Still, higher MTBR1 levels at baseline predicted faster rates of cognitive decline over the next nine years, suggesting the marker might be prognostic for dementia.
How did it track with tau pathology? In 280 CSF samples from the Copenhagen clinic, MBTR1 levels were higher in people who were amyloid-positive (A+) and higher still if a person had tested positive for p-tau217 (A+T+) as well (image below). CSF MTBR1 also distinguished A+/T+ from neurological controls with an AUC of 0.98. The controls included people who had frontotemporal or vascular dementia, dementia with Lewy bodies, and psychiatric disorders. As for Braak staging by tau PET, in 108 volunteers in the Gates cohort who had both CSF and tau PET data, CSF MTBR1 was significantly higher in Braak stage I-IV than in stage zero, and it was highest in Braak stages V and VI. CSF levels also correlated tightly with tau PET SUVR. eMTBR-243 also correlates best with Braak stages III and higher.

Tau Pathology or Neurodegeneration? People who test positive for amyloid and p-tau have more MTBR1 in their CSF. But so do people who had Creutzfeldt-Jacob disease. [Courtesy Gonzalez-Ortiz, University of Gothenburg.]
What exactly does this marker detect? Non-phosphorylated fragments of tau are known to increase in non-AD neurodegenerative conditions that lack neurofibrillary tangles, such as Creutzfeldt-Jacob disease, stroke, and traumatic brain injury (TBI). The scientists measured MTBR1 in the CSF of nine people with CJD who were admitted to the clinic in Copenhagen. Lo and behold, their levels were high as well, in one case more than threefold higher than in AD (image at left).
“This makes us wonder what MTBR1 measures,” said Gonzalez-Ortiz. “Would we see the same pattern if we used mass spectrometry, or is it just a facet of the immunoassay?” This will need to be tested, as will samples from TBI and stroke cases. For his part, Gonzalez-Ortiz believes the assay is a true reflection of the marker.
“Because it is positive in CJD, we think it more likely indicates neurodegeneration and is a peptide generated from total tau,” Blennow told Alzforum. He thinks it is advisable to test MTBR markers, including eMTBR-243, in people who have high levels of neurodegeneration but no tau pathology. “We do this because in our clinic we often get people referred to us with the question: Is this AD, or something acute, such as stroke or rapid neurodegeneration like CJD?” he said. Blennow suggested it would be good to ascertain that MTBR-243 peptide is not generated from total tau.
For his part, Horie conceded that he has not tested CJD for MTBR-243. In his hands, MTBR-243 tracks tightly with neurofibrillary tangles, while total tau accumulates in CJD due to massive neuron death. “We think CJD CSF contains mostly full-length, non-truncated tau,” he said.
Horie had his own questions about the U Gothenburg MTBR1 assay, namely whether it more closely reflects longer total tau forms than neurofibrillary tangles. “There are many species of MTBR tau, from the N-terminal to amino acid 243, and from 243 to the C-terminal side. We know that these N- and C-terminal fragments containing MTBR-243 do not associate with tangles,” he told Alzforum.
Indeed, when the WashU group measures MTBR-243, or eMTBR-243, they first immunodeplete long fragments that contain these epitopes, leaving only short MTBR fragments (image below). Gonzalez-Ortiz told Alzforum that he does not know how far the fragments detected by MTBR1 extend. “Since we don’t digest the samples, most likely we are capturing fragments of different lengths that contain the minimum required epitopes,” he wrote. “We are currently validating this using IP-MS to learn which of the endogenous fragments are the most common ones captured by the assay.”
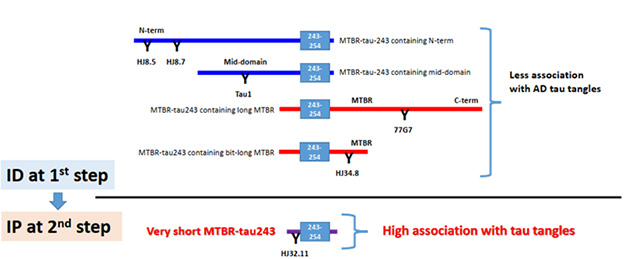
Immunodeplete First. Tau can be cleaved into many N-terminal and C-terminal fragments that contain the MTBR-243 region. WashU scientists immunodeplete these to leave only the small MTBR-243 domain, then immunoprecipitate that with the HJ32.11 antibody, before quantifying it by mass spectroscopy. [Courtesy of Kanta Horie, University of Washington.]
In Toronto, Horie and colleagues presented further evidence that MTBR-243 specifically tracks neurofibrillary tangles found in AD. They tested CSF samples from people clinically diagnosed with various neurodegenerative diseases, and in samples from people with pathologically confirmed diagnoses in collaboration with Adam Boxer at the University of California, San Francisco. The clinical cohort included 41 people. MTBR-243 was only elevated in people with AD and one person with frontotemporal dementia, who carried the R406W mutation. Fibrils in people with this mutation contain the same core fold that causes tangles in AD.
In the pathology cohort, a similar pattern emerged. AD CSF contained much higher MTBR-243 levels than did CSF from cognitively normal controls, but so did other samples. These included two people with progressive supranuclear palsy (PSP) and one with corticobasal syndrome (CBD)—all of whom turned out to have AD co-pathology. In addition, one person with FTLD-TDP43 had more MTBR-243 in their CSF than expected. This person had chronic traumatic encephalopathy as a co-pathology. Tau fibrils in CTE are known to adopt the same fold as in AD (Mar 2025 news). All told, the findings suggest that MTBR-243 specifically detects AD-like tau fibrils, which comprise tau isoforms that contain 3 and 4 repeats. In primary 3R tauopathies, such as Pick’s disease, or 4R tauopathies such as CBD, PSP, or argyrophilic grain disease, CSF MTBR-243 does not budge. “I think it is clear now that MTBR-243 is predictive of 3R/4R tau pathology,” said Horie. He believes this will help clinicians determine the underlying causes of a patient’s cognitive impairment, and help scientists monitor if tau therapies work.
The Phospho Variation
As for the MTBR-ptau262 assay developed by Gonzalez-Ortiz and colleagues, in Norwegian DDI CSF samples it also generated higher signals in people with brain amyloid (image below). As with MTBR1, people who had the most CSF MTBR-p262 at baseline declined fastest on cognitive tests during the next 11 years. In the Gates Ventures cohort, the MTBR-p262 level was higher in Braak stage I through IV than in stage zero, but was no higher in Braak V-VI.
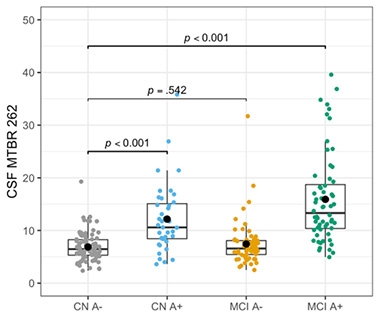
MTBR-p262 and Amyloid. In the DDI cohort, people who tested positive for amyloid had more MTBR-p262 in their CSF. Overlap was large. [Courtesy of Gonzalez-Ortiz, University of Gothenburg.]
As phospho-tau markers go, this one might be slightly different. While CSF p-tau181 and p-tau217 correlated tightly with each other, they correlated only moderately with CSF MTBR-p262. “It is possible that MTBR-p262 reflects something else,” said Gonzalez-Ortiz.
Horie believes this marker could be very interesting. “Amino acid 262 sits near the tangle core, so it will be important to see more data on its association with tangles,” he said. He thinks this marker might not increase continuously as disease progresses because it could get subsumed into maturing tangles. “It might show a bell-shaped trajectory,” he suggested. Whether that explains the weak correlation with p-tau217 and p-tau181 remains to be determined.
Gonzalez-Ortiz has begun to tweak this immunoassay for use in plasma. Preliminary data suggest that most samples fall below the lower limit of quantification. But any time he did detect a signal, it was in samples that came from people who had AD. He plans to optimize the assay to make it more sensitive.—Tom Fagan
References
News Citations
- Will We Soon Stage Alzheimer’s With Plasma Markers?
- Better Diagnosis with Blood Test Detecting Only Tau Made in Brain
- Filling in the Family Tree: AD, CTE Folds Spotted in Other Tauopathies
Mutations Citations
Further Reading
No Available Further Reading
Annotate
To make an annotation you must Login or Register.
Comments
Washington University School of Medicine
In human CSF, there are various forms (lengths) of MTBR-tau species containing the residue 243 (MTBR-tau243). Since MTBR-tau243 species specific to AD tau tangles are short, our original method to quantify the tryptic MTBR-tau243 peptide (243-254) by mass spectrometry included purification steps, consisting of immunodepletion of long MTBR-tau fragments using anti-N-terminal tau antibodies (HJ8.5 and HJ8.7), anti-mid-domain tau antibody (Tau1), and anti-late-R1 antibody (HJ34.8). Then we immunoprecipitated short MTBR-tau fragments using antibody (HJ32.11) (Horie et al., 2023) that binds upstream of R1. Unless these purification steps are included, the MTBR-tau243 biomarker cannot be used to identify AD tau pathology.
In case of a simple sandwich ELISA system, using two linear-epitope antibodies, with no purification step as described above, I would expect that the assay would behave as a total-tau biomarker.
Recently, we developed a blood-based biomarker, plasma MTBR-tau243, to identify AD tau pathology (Horie et al., 2025). In this new plasma method, we utilized a simple one-step immunoprecipitation procedure using HJ32.11, followed by the quantification of the endogenous MTBR-tau243 species (called as “eMTBR-tau243”) ending at residue 256 (V) and deamidated at residue 255 (N). Both the original CSF method and the new CSF/plasma eMTBR-tau243 method can predict AD tau pathology accurately.
However, to be precise, the MTBR-tau243 species quantified by both methods are different from each other. In the literature, we showed that plasma eMTBR-tau243 (ending at the residue 256) is more predictive for tau-PET SUVR in the intermediate to late tau pathological regions (i.e., Braak III-VI regions) than early region (e.g., Braak I-II) in AD, while the original CSF MTBR-tau243 could accurately predict the tau-PET SUVR from temporal meta-ROI (i.e., Braak I–IV). It is important to deeply understand the characteristics of MTBR-tau243 for the appropriate use to predict AD tau pathology.
References:
Horie K, Salvadó G, Barthélemy NR, Janelidze S, Li Y, He Y, Saef B, Chen CD, Jiang H, Strandberg O, Pichet Binette A, Palmqvist S, Sato C, Sachdev P, Koyama A, Gordon BA, Benzinger TL, Holtzman DM, Morris JC, Mattsson-Carlgren N, Stomrud E, Ossenkoppele R, Schindler SE, Hansson O, Bateman RJ. CSF MTBR-tau243 is a specific biomarker of tau tangle pathology in Alzheimer's disease. Nat Med. 2023 Aug;29(8):1954-1963. Epub 2023 Jul 13 PubMed.
Horie K, Salvadó G, Koppisetti RK, Janelidze S, Barthélemy NR, He Y, Sato C, Gordon BA, Jiang H, Benzinger TL, Stomrud E, Holtzman DM, Mattsson-Carlgren N, Morris JC, Palmqvist S, Ossenkoppele R, Schindler SE, Hansson O, Bateman RJ. Plasma MTBR-tau243 biomarker identifies tau tangle pathology in Alzheimer's disease. Nat Med. 2025 Jun;31(6):2044-2053. Epub 2025 Mar 31 PubMed.
Make a Comment
To make a comment you must login or register.