Occipital Amyloid: Giveaway for ARIA Risk?
Quick Links
While amyloid immunotherapy is slowly becoming more accepted in clinical use, its biggest drawback remains the risk of ARIA. Scientists continue to study which patients are most at risk, how to identify them earlier, and how to make the treatments safer.
At the Alzheimer’s Association International Conference, held July 27-31 in Toronto, Ian Kennedy of Eli Lilly made a case for a heavy occipital amyloid load flagging higher risk. Lilly’s Hong Wang presented 18-month data for the company’s modified titration of donanemab, firming up the conclusion that a slower ramp-up cuts ARIA-E risk by a third.
- High occipital amyloid burden nearly doubles the odds of ARIA-E.
- Stepwise titration of donanemab confirmed to cut ARIA-E risk by a third.
- Clinical programs continue to report low rates of ARIA-E.
Meanwhile, talks from clinicians consistently reported that ARIA rates during real-world lecanemab treatment are the same or slightly better than in trials, at least among programs that chose to present their results in Toronto. On August 28, the U.S. Food and Drug Administration updated lecanemab’s label to require an additional MRI safety scan between the second and third infusions in order to catch ARIA earlier.
In other lecanemab news, on August 29 the FDA approved the subcutaneous formulation for maintenance dosing (see company press release and Aug 2025 conference news on this strategy).
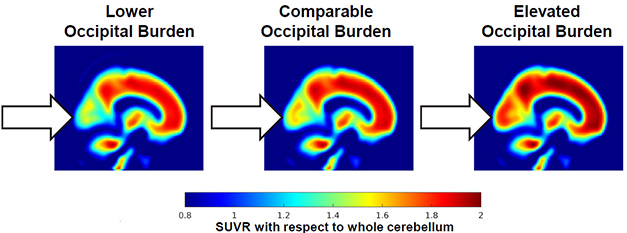
Danger Sign? About a third of people with amyloid plaques have scant amyloid (left) in the occipital cortex (arrows), about a third have the same amount as in the rest of the brain (middle), and a third have elevated amyloid there (right). The latter two conditions are linked to a higher risk of ARIA-E. [Courtesy of Eli Lilly.]
Is Occipital Amyloid Especially Bad For You?
Trial data show that the more Aβ a person has in their brain, the higher their risk of ARIA-E (Nov 2023 conference news; Zimmer et al., 2025). In clinical use, too, people at later disease stages, with higher plaque loads, get more edema (May 2025 news).
Kennedy homed in on occipital amyloid because data from the Graduate trials of gantenerumab implicated this region in particular (Salloway et al., 2025). Potentially, this is because occipital amyloid is strongly associated with cerebral amyloid angiopathy, a known risk factor for ARIA, Kennedy said in Toronto (Nelson et al., 2013; Aug 2023 conference news; Aug 2024 conference news).
To test occipital amyloid’s effect, Kennedy analyzed data from participants in three donanemab trials: 131 people from the Phase 2 study, 1,885 from Phase 3, and 71 people from a head-to-head study of donanemab and aducanumab. All 2,087 received donanemab, and all had amyloid PET scans, most with florbetapir and a few with florbetaben. Kennedy categorized each person as having low, comparable, or elevated occipital amyloid compared with their global burden. He found many people in each category, with 741 people having low, 561 comparable, and 785 elevated occipital amyloid (image above).
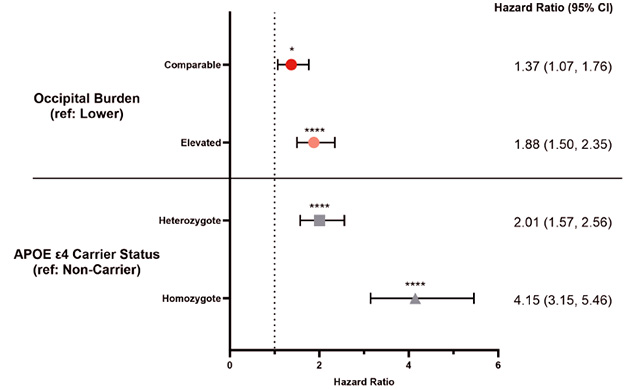
New Risk Factor? Having elevated occipital amyloid (orange) raised ARIA-E risk as much as having one APOE4 allele (gray square) did. Even moderate occipital amyloid (red) significantly boosted risk. [Courtesy of Eli Lilly.]
Kennedy then linked occipital amyloid load to ARIA-E incidence. Judged against those with a low burden, having a comparable occipital burden pushed up risk by 40 percent, and a high burden elevated it by 90. As expected, APOE genotype had an even stronger effect, with one APOE4 allele doubling ARIA-E risk, and two alleles quadrupling it (image above). Importantly, the effects of occipital amyloid and APOE4 were independent of each other, suggesting that measures of occipital amyloid could add value to risk assessments. More research is needed to quantify and validate this finding, Kennedy noted.
Slower Titration Wins the Day
Lilly scientists have found one simple way to lower ARIA-E risk: step up dosing more gradually. Previously, at this year’s AD/PD in Vienna, the company had presented one-year data from its Trailblazer-Alz6 trial of different titration schemes, reporting that a slower ramp-up significantly curtailed ARIA-E incidence (May 2025 conference news; Wang et al., 2025).
In Toronto, Wang showed final data from this 18-month trial. The bottom line? Not much changed from 12 months. ARIA-E numbers were identical to those at one year, because no additional cases occurred in the 212 participants between 12 and 18 months. In the final analysis, the slower titration cut ARIA-E incidence by a third, bringing it down to 16 percent, close to lecanemab’s reported 13 percent. The biggest change was for APOE4 homozygotes, whose risk more than halved, from 57 to 24 percent. This rate is less than in the lecanemab Clarity Phase 3 trial, where homozygotes had a 32 percent incidence.
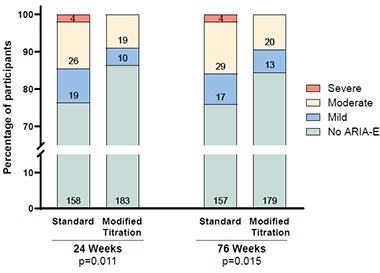
Milder ARIA-E. On a stepwise donanemab titration schedule, there were fewer severe (red) and moderate (beige) cases of ARIA-E than with standard titration at both six months (left) and 18 months (right). Numbers of cases in each category are listed on bars. [Courtesy of Eli Lilly.]
When ARIA-E did occur, it was milder. There were no radiologically severe cases, compared with four among the 207 people on standard donanemab titration. There were also a third fewer moderate cases on the slower titration (image at right). The incidence of symptomatic ARIA-E dropped from 5 to 3 percent, though the difference was not statistically significant.
Regarding ARIA-H, overall risk did not change, but superficial siderosis dropped by a third. These cortical iron deposits indicate brain bleeds, and are considered more serious than the more common microhemorrhages. There was also a third less concurrent ARIA-E and -H (Wang et al., 2025).
The modified titration has been approved for use in the U.S., Australia, and Singapore so far, with applications pending in several other countries (Jul 2025 community news).
Is There Less ARIA-E in Real-world Use?
In Toronto, several clinicians discussed safety data from the first patients at their centers to take lecanemab. Patient numbers at each center remain quite low, from a few dozen to several hundred. Most of these specialty clinics follow the appropriate-use recommendations for lecanemab and donanemab, which are more stringent than the trial exclusion criteria or the FDA label (Apr 2023 conference news; Nov 2024 conference news). Perhaps as a result of this, ARIA-E rates appear lower than in trials.
David Weisman of Abingdon Neurology Associates, Pennsylvania, presented interim findings from an Eisai-sponsored study at nine clinical sites in the U.S. Among the 178 participants treated so far, 8 percent developed ARIA-E, and 1 percent had symptoms. There were no radiologically severe cases. Marwan Sabbagh of the Barrow Neurological Institute in Phoenix broke this out by genotype. The 30 APOE4 homozygotes had a 13 percent ARIA-E rate, with 3 percent symptomatic and no severe cases. In Clarity, 13 percent of participants had ARIA-E and 3 percent had symptoms overall, with homozygotes having a 32 percent incidence.
Other small programs reported similar numbers. Alison O’Donnell of the VA Pittsburgh Healthcare System said the 32 veterans taking lecanemab there notched a 9 percent ARIA-E incidence. Wenjun Wang of Peking Union Medical College Hospital in Beijing reported a 7 percent ARIA-E incidence among 29 patients, with all cases radiologically mild and asymptomatic. He ascribed the low rate to how carefully physicians selected patients who were appropriate for the therapy.
Likewise, Michael Rosenbloom of the University of Washington, Seattle, reported a 9 percent ARIA-E rate among 79 patients treated at an academic practice, the UW Harborview Medical Center, and a 7 percent rate among 95 patients treated at a private neurology practice, Abington Neurological Associates. Larry Honig of Columbia University, New York City, discussed data from a somewhat larger program. Of the 239 patients treated at Columbia so far, 11 percent have had ARIA-E. Among 26 APOE4 homozygotes, the rate was 27 percent.
An audience member wondered if lessened ARIA rates in clinical practice could be due to missed diagnoses because many such sites use lower field strength MRIs compared with trials. Rosenbloom thinks this could make a difference. He noted that UW-HMC reported a 10 percent ARIA-H rate, versus 2 percent at Abington. Rosenbloom attributed this to the use of 3T MRI and susceptibility-weighted imaging at UW-HMC, compared with a combination of 1.5T and 3T MRI at Abington. SWI is particularly good for spotting ARIA-H.
However, detection technology in clinics is not necessarily worse than that used in trials, said Suzanne Schindler at Washington University, St. Louis. She noted that the Clarity trial employed gradient echo MRI sequences to spot ARIA-H, and most specialty clinics use SWI, which is three times more sensitive. “We can’t assume that clinics are missing cases,” Schindler said in Toronto.
Regarding ARIA-E, Weisman agreed lower field strength could lead clinicians to miss mild cases, but noted that moderate or severe cases would still show up. Mild, asymptomatic cases are of the least concern clinically, with many centers choosing to continue dosing for these patients.
A recent paper adds some numbers to this. Scientists led by Jeffrey Petrella at Duke University School of Medicine in Durham, North Carolina, determined that radiologists missed half of mild ARIA-E cases and 40 percent of mild ARIA-H compared with AI-assisted reads. Use of AI tools could improve detection and management of this symptom, they concluded (Petrella et al., 2025). One such tool, icobrain aria, was recently approved by the U.S. Food and Drug Administration based on these data (Nov 2024 news).
Main Symptom? Headache
What about other safety signals? In Toronto, Jay Lusk of the University of North Carolina, Chapel Hill, described a study of electronic health records from July 2023, when lecanemab received traditional approval, through the end of 2024. In this dataset, 555 people had used lecanemab or donanemab, versus more than a million controls who had not.
Comparing health outcomes between the two groups after a year, Lusk found that people on amyloid immunotherapy had about double the incidence of headaches compared with controls, and a 50 percent higher risk of respiratory infections. There were no other safety signals, with no increased risk of intracerebral hemorrhage, heart attack, or stroke. This dataset did not include ARIA incidence. Lusk called the findings reassuring.
Weisman noted that when the Centers for Medicare and Medicaid Services initially denied coverage for amyloid immunotherapies in 2022, CMS administrators expressed concern that clinicians would prescribe the drugs to inappropriate patients and/or not adequately monitor safety (Apr 2022 community news). “The data show that’s not happening,” Weisman wrote to Alzforum.
Indeed, many clinicians have been quite conservative in their choice of whom to treat, steering away patients they considered at higher risk. Early experiences with the drugs have allowed clinicians to relax a bit, Rosenbloom noted. “At first we followed the appropriate-use recommendations to the letter, now we’re more comfortable in using judgment,” he said in Toronto.—Madolyn Bowman Rogers
References
Therapeutics Citations
News Citations
- First Morsel of Results from DIAN Concurrent Amyloid and Tau Trial
- Unlocking Blood-Brain Barrier Boosts Immunotherapy Efficacy, Lowers ARIA
- In Clinical Use, Most ARIA Occurs in People With Dementia, Not MCI
- Is ARIA an Inflammatory Reaction to Vascular Amyloid?
- Implicated in ARIA: Perivascular Macrophages and Microglia
- Next Act for Amyloid Immunotherapy: Be Safer, Target Tau, Too
- FDA Approves Safer, Slower Donanemab Titration
- Next Goals for Immunotherapy: Make It Safer, Less of a Hassle
- Donanemab: Small Tweak in Titration, Big Gain in Safety?
- AI to Spot ARIA? FDA Says Yes
- Drilling Down into the CMS Aduhelm Decision—A Primer
Paper Citations
- Zimmer JA, Ardayfio P, Wang H, Khanna R, Evans CD, Lu M, Sparks J, Andersen S, Lauzon S, Nery ES, Battioui C, Engle SE, Biffi A, Svaldi D, Salloway S, Greenberg SM, Sperling RA, Mintun M, Brooks DA, Sims JR. Amyloid-Related Imaging Abnormalities With Donanemab in Early Symptomatic Alzheimer Disease: Secondary Analysis of the TRAILBLAZER-ALZ and ALZ 2 Randomized Clinical Trials. JAMA Neurol. 2025 May 1;82(5):461-469. PubMed.
- Salloway S, Wojtowicz J, Voyle N, Lane CA, Klein G, Lyons M, Rossomanno S, Mazzo F, Bullain S, Barkhof F, Bittner T, Schneider A, Grundman M, Aldea R, Boada M, Smith J, Doody R. Amyloid-Related Imaging Abnormalities (ARIA) in Clinical Trials of Gantenerumab in Early Alzheimer Disease. JAMA Neurol. 2025 Jan 1;82(1):19-29. PubMed.
- Nelson PT, Pious NM, Jicha GA, Wilcock DM, Fardo DW, Estus S, Rebeck GW. APOE-ε2 and APOE-ε4 correlate with increased amyloid accumulation in cerebral vasculature. J Neuropathol Exp Neurol. 2013 Jul;72(7):708-15. PubMed.
- Wang H, Serap Monkul Nery E, Ardayfio P, Khanna R, Otero Svaldi D, Gueorguieva I, Shcherbinin S, Andersen SW, Hauck PM, Engle SE, Brooks DA, Collins EC, Fox NC, Greenberg SM, Salloway S, Mintun MA, Sims JR. Modified titration of donanemab reduces ARIA risk and maintains amyloid reduction. Alzheimers Dement. 2025 Apr;21(4):e70062. PubMed.
- Wang H, Nery ES, Ardayfio P, Khanna R, Svaldi DO, Shcherbinin S, Xu W, Andersen SW, Hauck PM, Brooks DA, Collins EC, Salloway S, Mintun MA, Sims JR. The effect of modified donanemab titration on amyloid-related imaging abnormalities with edema/effusions and amyloid reduction: 18-month results from TRAILBLAZER-ALZ 6. J Prev Alzheimers Dis. 2025 Jul 5;:100266. Epub 2025 Jul 5 PubMed.
- Petrella JR, Liu AJ, Wang LA, Doraiswamy PM. AI-Assisted Detection of Amyloid-related Imaging Abnormalities (ARIA): Promise and Pitfalls. AJNR Am J Neuroradiol. 2025 Jul 30; Epub 2025 Jul 30 PubMed.
External Citations
Further Reading
Annotate
To make an annotation you must Login or Register.
Comments
No Available Comments
Make a Comment
To make a comment you must login or register.