Troubling Trend? Cytotoxic T cells Swarm Midbrain in PSP
Quick Links
At the AD/PD meeting held last month in Vienna, scientists implicated T lymphocytes—specifically, the cytotoxic, CD8-positive variety—in Alzheimer’s disease. While the modus operandi of these cells in neurodegenerative disease is far from settled, T cell-targeted therapies are already in early clinical trials (Apr 2025 news; Apr 2025 news). Lost in the conference shuffle was yet another report of misbegotten T cells. This time, the cells had reportedly flocked into the tauopathy-ravaged midbrains of people with progressive supranuclear palsy (PSP). Led by Gabor Kovacs of the University of Toronto and published April 15 in Brain, this neuropathological study reported far fewer of these infiltrators in the midbrains of people with Parkinson’s disease.
- Neuropathology study spots CD8+ T cells in the brains of people with PSP.
- The cells were scarce in the brains of controls or in people with Parkinson’s.
- The findings add to recent evidence implicating the cells in Alzheimer’s disease.
Scientists are catching on to a potential role of invading T cells in neurodegenerative disease, as seen by an uptick in studies published on the topic. One group spotted CD8+ T cells in the CSF and brains of people with AD and PD, where the cells appeared to have multiplied in response to specific antigens (Jan 2020 news; Dec 2022 news). Another reported CD8+ T cell infiltration in the substantia nigra in early phases of PD, while yet another saw CD4+ T-helper cells lurking near Lewy bodies (Galiano-Landeira et al., 2020; Oct 2021 news). In cases of FTLD-tau, CD8+ T cells were found in the frontal cortex, where their numbers correlated with the extent of a person’s tau pathology (Hartnell et al., 2024).
To look in PSP, a 4R-tauopathy, first author Blas Couto and colleagues compared sections of the midbrain from nine people with this disease, 10 with PD, and six controls. The midbrain, particularly the substantia nigra, is a hotspot for tau tangle pathology in PSP and for α-synuclein pathology in PD. The authors immunostained the brain samples with antibodies specific for phosphorylated tau, α-synuclein, the cytotoxic T cell marker CD8, and the microglial marker HLA-DR, then used stereology software to examine closely how these markers associated with one another.
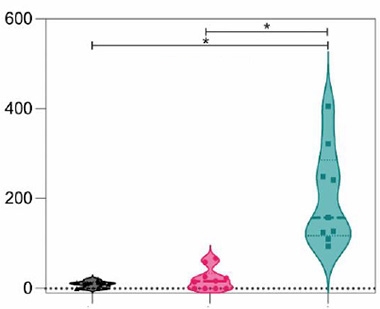
Killer Component. Far more CD8+ T cells per cubic millimeter (Y axis) were spotted in the substantia nigra of people with PSP (cyan) than those with PD (pink) or controls (gray). [Courtesy of Couto et al., Brain, 2024.]
The scientists found far more nigral CD8+ T cells in people with PSP than in those with PD or controls. Even the PSP sample with the fewest CD8+ T cells was inundated with more of the cells than any of the PD or control samples (image above). The same held true in other subregions of the midbrain, where PSP samples had the most CD8+ T cells.
In four of the PSP samples, the scientists saw T cells in close contact with neurons, suggesting that they could have been in the process of killing (image below). The extent of the CD8 invasion did not appear to track with the severity of disease, as judged by how long each person had lived after disease onset.
People with PSP also had more microglia mingling in their substantia nigra than those with PD or controls, which housed similar numbers of microglia. These microglial numbers did not track with T cell counts, but did correlate with a younger age at death among people with PSP.
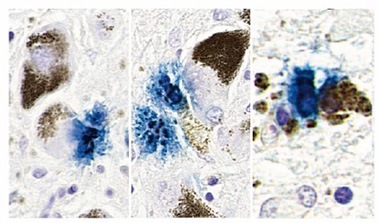
Deadly Contact? Immunostaining implied close contact between CD8+ T cells (blue) and neurons (brown, neuromelanin). Different examples from one PSP sample are shown. [Courtesy of Couto et al., Brain, 2024.]
As expected, the load of neurofibrillary tau tangles in the midbrain was far higher in people with PSP than those with PD, while people with PD had more α-synuclein Lewy bodies. Importantly, perhaps, neither type of neuropathology tracked with numbers of CD8+ T cells within any subregion of the midbrain examined. That said, CD8+ T cells were scarcely seen in regions with little to no pathology, such as the cortex.
Postmortem sightings cannot nail down how the CD8+ T cells influenced the disease process. Even so, Kovacs suspects the cells were making things worse. “Since the appearance of CD8 cells is higher in brain regions that are more severely degenerating and causing the symptoms, our findings support the notion that CD8 cells are detrimental,” Kovacs wrote to Alzforum. Furthermore, direct contact between CD8+ T cells and neurons—which was seen in some of the PSP samples—is a dead giveaway that cytotoxic T cells are doing their dirty work. Kovacs said that some neurons appeared to have multiple contact points with the killer cells, a phenomenon commonly seen in autoimmune disorders. He thinks it’s possible that at least some cases of PSP have an autoimmune component.
The findings jibe with those of a recent neuropathology study by Finnish, Danish, and Austrian researchers, who also spotted CD8s in the midbrain of PSP patients (Backman et al., 2025). That study’s leader, Valtteri Kaasinen of the University of Turku in Finland, agreed with Kovacs’ interpretation that the cells were likely detrimental.
“Although causality remains to be firmly established, the presence of CD8+ T cells in regions of neurodegeneration raises the possibility that PSP may, at least in part, have an immunological component,” Kaasinen wrote to Alzforum. “This would align it with a broader trend across neurodegenerative diseases, where adaptive immune responses are increasingly implicated.”
Kovacs noted that the small numbers of CD8+ T cells observed in the SNs of people with PD does not rule out a role for the cells in that disease, too. It could be that the cells are involved earlier in disease, as reported previously, or that their numbers are smaller due to an overall lower burden of α-synuclein pathology in PD relative to the burden of NFTs in PSP. PSP is a more rapidly progressing disease than PD.
Kovacs noted that his group’s analysis adds another tauopathy, besides AD, to diseases marked by CD8+ T cell infiltration. “We cannot conclude based on our study whether misfolded tau induced the CD8 response, or whether an autoimmune process led to the misfolding of tau,” he wrote.—Jessica Shugart
References
News Citations
- Killers in the Crosshairs: Zeroing in on Invading CD8+ T Cells
- Therapies Aim to Tame T Cells in the Brain
- Attack of the Clones? Memory CD8+ T Cells Stalk the AD, PD Brain
- In AD, CSF Immune Cells Hint at Mounting Mayhem in the Brain
- Intruder Alert: Inflammatory T Cells Lurk Near Lewy Bodies, Neurons
Paper Citations
- Galiano-Landeira J, Torra A, Vila M, Bové J. CD8 T cell nigral infiltration precedes synucleinopathy in early stages of Parkinson's disease. Brain. 2020 Dec 1;143(12):3717-3733. PubMed.
- Hartnell IJ, Woodhouse D, Jasper W, Mason L, Marwaha P, Graffeuil M, Lau LC, Norman JL, Chatelet DS, Buee L, Nicoll JA, Blum D, Dorothee G, Boche D. Glial reactivity and T cell infiltration in frontotemporal lobar degeneration with tau pathology. Brain. 2024 Feb 1;147(2):590-606. PubMed.
- Backman EA, Gardberg M, Luntamo L, Peurla M, Vahlberg T, Borghammer P, Stefanova N, Wenning G, Kaasinen V. Nigral Neuroinflammation and Dopaminergic Neurons in Parkinson's Disease and Atypical Parkinsonisms. Ann Neurol. 2025 Feb 7; Epub 2025 Feb 7 PubMed.
Further Reading
No Available Further Reading
Primary Papers
- Couto B, Forrest SL, Fearon C, Lee S, Knott S, Li J, Fox SH, Tartaglia MC, Lang AE, Kovacs GG. Midbrain cytotoxic T cells as a distinct neuropathological feature of progressive supranuclear palsy. Brain. 2025 Aug 1;148(8):2650-2657. PubMed.
Annotate
To make an annotation you must Login or Register.
Comments
University of Turku
The new findings highlighting CD8+ T cell abundance in the PSP midbrain are highly intriguing and, in my view, consistent with a growing body of evidence pointing toward immune dysregulation in atypical parkinsonian syndromes. In our recent study (Backman et al., 2025), we also observed markers of T cell-related inflammation in the midbrain, suggesting that CD8+ T cells may not merely be bystanders but could actively contribute to disease pathogenesis.
Although causality remains to be firmly established, the presence of CD8+ T cells in regions of neurodegeneration raises the possibility that PSP may, at least in part, have an immunological component. This would align it with a broader trend across neurodegenerative diseases, where adaptive immune responses are increasingly implicated.
In the long term, if these findings are validated, they may open new therapeutic avenues. Immunomodulatory strategies could eventually be repurposed or tailored for PSP, which thus far lacks disease-modifying treatments.
References:
Backman EA, Gardberg M, Luntamo L, Peurla M, Vahlberg T, Borghammer P, Stefanova N, Wenning G, Kaasinen V. Nigral Neuroinflammation and Dopaminergic Neurons in Parkinson's Disease and Atypical Parkinsonisms. Ann Neurol. 2025 Feb 7; Epub 2025 Feb 7 PubMed.
Houston Methodist
This study provides new evidence supporting the contribution of the systemic adaptive immune system—particularly the CD8+ T cell population—to the pathophysiology of PSP. Previous studies have reported a role of cytotoxic CD8+ T cells in other neurodegenerative disorders, including Alzheimer’s disease, amyotrophic lateral sclerosis, and frontotemporal dementia, highlighting CD8+ T cell–mediated cytotoxicity as a potentially shared mechanism across neurodegenerative conditions.
Although the exact mechanism by which peripheral CD8⁺ T cells infiltrate the brain remains unclear, one possible explanation is that persistent glial activation in the presence of proteinopathy triggers the release of inflammatory cytokines and chemokines, which in turn activate and recruit peripheral cytotoxic T cells to sites of pathology, thereby exacerbating glial activation and/or exerting direct neurotoxic effects.
Modification of cytotoxic T cells has preserved brain tissue in a taupathy preclinical mouse model (Chen et al., 2023). If this hypothesis is validated, it could open new avenues for therapeutic intervention. We have been advancing novel immunotherapeutic strategies to target adaptive immune system in neurodegenerative disorders, including low-dose IL-2 therapy (Faridar et al., 2023) to expand regulatory T cells, and combination therapies with IL-2 and CTLA-4 IgG (Thonhoff et al., 2024) to target both Tregs and cytotoxic immune subpopulations. These approaches may offer promising avenues for modifying and restoring adaptive immune responses and mitigating central inflammation in taupathies including PSP.
References:
Chen X, Firulyova M, Manis M, Herz J, Smirnov I, Aladyeva E, Wang C, Bao X, Finn MB, Hu H, Shchukina I, Kim MW, Yuede CM, Kipnis J, Artyomov MN, Ulrich JD, Holtzman DM. Microglia-mediated T cell infiltration drives neurodegeneration in tauopathy. Nature. 2023 Mar;615(7953):668-677. Epub 2023 Mar 8 PubMed. Correction.
Faridar A, Eid AM, Thome AD, Zhao W, Beers DR, Pascual MB, Nakawah MO, Roman GC, Davis CS, Grundman M, Masdeu JC, Appel SH. A phase 1 open-label pilot study of low-dose interleukine-2 immunotherapy in patients with Alzheimer's disease. Transl Neurodegener. 2023 Nov 16;12(1):54. PubMed.
Thonhoff JR, Beers DR, Zhao W, Faridar A, Thome A, Wen S, Zhang A, Wang J, Appel SH. A phase 1 proof-of-concept study evaluating safety, tolerability, and biological marker responses with combination therapy of CTLA4-Ig and interleukin-2 in amyotrophic lateral sclerosis. Front Neurol. 2024;15:1415106. Epub 2024 Jun 10 PubMed.
Make a Comment
To make a comment you must login or register.